10-K: Annual report pursuant to Section 13 and 15(d)
Published on February 29, 2016
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, DC 20549
FORM 10-K
(Mark One)
ý |
ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the fiscal year ended December 31, 2015.
OR
o |
TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the transition period from to .
Commission file number 001-33528
OPKO Health, Inc.
(Exact Name of Registrant as Specified in Its Charter)
Delaware |
75-2402409 |
|
|
(State or Other Jurisdiction of
Incorporation or Organization)
|
(I.R.S. Employer
Identification No.)
|
|
4400 Biscayne Blvd., Miami, FL 33137 (Address of Principal Executive Offices) (Zip Code) |
(Registrant’s Telephone Number, Including Area Code): (305) 575-4100
|
Securities registered pursuant to section 12(b) of the Act: | ||
Title of Each Class |
Name of Each Exchange on Which Registered |
|
Common Stock, $.01 par value per share |
New York Stock Exchange |
|
Securities registered pursuant to section 12(g) of the Act:
None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ý No ¨
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes ¨ No ý
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes ý No ¨
Indicate by check mark whether the Registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes ý No ¨
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. ¨
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definitions of “large accelerated filer,” “accelerated filer” and “smaller reporting company” in Rule 12b-2 of the Exchange Act.
(in Rule 12b-2 of the Exchange Act) (Check one): |
|||
Large accelerated filer |
ý |
Accelerated filer |
o |
Non-accelerated filer |
o (Do not check if a smaller reporting company)
|
Smaller reporting company |
o |
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Act). Yes ¨ No ý
The aggregate market value of the voting and non-voting common equity held by non-affiliates computed by reference to the price at which the common equity was last sold, as of the last business day of the registrant’s most recently completed second fiscal quarter was: $3,877,294,326.
As of February 16, 2016, the registrant had 545,696,849 shares of Common Stock outstanding.
Documents Incorporated by Reference
Portions of the registrant’s definitive proxy statement for its 2016 Annual Meeting of Stockholders are incorporated by reference in Items 10, 11, 12, 13, and 14 of Part III of this Annual Report on Form 10-K.
TABLE OF CONTENTS
Page |
|||
Part I. |
|||
Item 1. |
|||
Item 1A. |
|||
Item 1B. |
|||
Item 2. |
|||
Item 3. |
|||
Item 4. |
|||
Part II. |
|||
Item 5. |
|||
Item 6. |
|||
Item 7. |
|||
Item 7A. |
|||
Item 8. |
|||
Item 9. |
|||
Item 9A. |
|||
Item 9B. |
|||
Part III. |
|||
Item 10. |
Directors, Executive Officers and Corporate Governance |
||
Item 11. |
Executive Compensation |
||
Item 12. |
Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters |
||
Item 13. |
Certain Relationships and Related Transactions and Director Independence |
||
Item 14. |
Principal Accounting Fees and Services |
||
Part IV. |
|||
Item 15. |
|||
Signatures |
|||
Certifications |
|||
EX-21 |
|||
EX-23.1 |
|||
EX-23.2 |
|||
EX-31.1 |
|||
EX-31.2 |
|||
EX-32.1 |
|||
EX-32.2 |
|||
EX-101. INS XBRL Instance Document |
|||
EX-101.SCH XBRL Taxonomy Extension Schema Document |
|||
EX-101.CAL XBRL Taxonomy Extension Calculation Linkbase Document |
|||
EX-101.DEF XBRL Taxonomy Extension Definition Linkbase Document |
|||
EX-101.LAB XBRL Taxonomy Extension Label Linkbase Document |
|||
EX-101.PRE XBRL Taxonomy Extension Presentation Linkbase Document |
|||
3
CAUTIONARY STATEMENT REGARDING FORWARD-LOOKING STATEMENTS
This Annual Report on Form 10-K contains “forward-looking statements,” as that term is defined under the Private Securities Litigation Reform Act of 1995 (“PSLRA”), Section 27A of the Securities Act of 1933, as amended, and Section 21E of the Securities Exchange Act of 1934, as amended. Forward-looking statements include statements about our expectations, beliefs or intentions regarding our product development efforts, business, financial condition, results of operations, strategies or prospects. You can identify forward-looking statements by the fact that these statements do not relate strictly to historical or current matters. Rather, forward-looking statements relate to anticipated or expected events, activities, trends or results as of the date they are made. Because forward-looking statements relate to matters that have not yet occurred, these statements are inherently subject to risks and uncertainties that could cause our actual results to differ materially from any future results expressed or implied by the forward-looking statements. Many factors could cause our actual activities or results to differ materially from the activities and results anticipated in forward-looking statements. These factors include those described below and in “Item 1A-Risk Factors” of this Annual Report on Form 10-K. We do not undertake an obligation to update forward-looking statements. We intend that all forward-looking statements be subject to the safe-harbor provisions of the
PSLRA. These forward-looking statements are only predictions and reflect our views as of the date they are made with respect to future events and financial performance.
Risks and uncertainties, the occurrence of which could adversely affect our business, include the following:
• |
we have a history of losses and may not become profitable in the near future; |
• |
the risks inherent in funding, developing and obtaining regulatory approvals of new, commercially-viable and competitive products and treatments; |
• |
our research and development activities may not result in commercially viable products; |
• |
that earlier clinical results of effectiveness and safety may not be reproducible or indicative of future results; |
• |
that we may fail to obtain regulatory approval for or successfully commercialize Rayaldee and hGH-CTP;
|
• |
that we may not generate profits or cash flow from our laboratory operations or substantial revenue from our diagnostic products; |
• |
that currently available over-the-counter and prescription products, as well as products under development by others, may prove to be as or more effective than our products for the indications being studied; |
• |
our ability to develop a pharmaceutical sales and marketing infrastructure; |
• |
our ability and our distribution and marketing partners’ ability to comply with regulatory requirements regarding the sales, marketing and manufacturing of our products and product candidates and the operation of our laboratories; |
• |
the performance of our third-party distribution partners, licensees and manufacturers over which we have limited control; |
• |
our success is dependent on the involvement and continued efforts of our Chairman and Chief Executive Officer; |
• |
integration challenges for Bio-Reference, EirGen and other acquired businesses; |
• |
changes in regulation and policies in the United States and other countries, including increasing downward pressure on health care reimbursement; |
• |
our ability to manage our growth and our expanded operations; |
• |
increased competition, including price competition; |
• |
changing relationships with payers, including the various state and multi-state Blues programs, suppliers and strategic partners; |
• |
efforts by third-party payors to reduce utilization and reimbursement for clinical testing services; |
• |
failure to timely or accurately bill for our services; |
• |
failure to obtain and retain new clients and business partners, or a reduction in tests ordered or specimens submitted by existing clients; |
• |
failure to establish, and perform to, appropriate quality standards to assure that the highest level of quality is observed in the performance of our testing services; |
• |
failure to maintain the security of patient-related information; |
• |
our ability to obtain and maintain intellectual property protection for our products; |
• |
our ability to defend our intellectual property rights with respect to our products; |
• |
our ability to operate our business without infringing the intellectual property rights of others; |
• |
our ability to attract and retain key scientific and management personnel; |
• |
our need for, and ability to obtain, additional financing; |
• |
adverse results in material litigation matters or governmental inquiries; |
• |
failure to obtain and maintain regulatory approval outside the U.S.; and |
• |
legal, economic, political, regulatory, currency exchange, and other risks associated with international operations; |
4
PART I
Unless the context otherwise requires, all references in this Annual Report on Form 10-K to the “Company”, “OPKO”, “we”, “our”, “ours”, and “us” refer to OPKO Health, Inc., a Delaware corporation, including our wholly-owned subsidiaries.
ITEM 1. |
BUSINESS |
OVERVIEW
We are a diversified healthcare company that seeks to establish industry-leading positions in large and rapidly growing medical markets. Our diagnostics business includes Bio-Reference Laboratories (“Bio-Reference”), the nation’s third-largest clinical laboratory with a core genetic testing business and a 420-person sales force to drive growth and leverage new products, including the 4Kscore prostate cancer test and the Claros 1 in-office immunoassay platform. Our pharmaceutical business features Rayaldee, a treatment for secondary hyperparathyroidism (“SHPT”) in patients with stage 3 or 4 chronic kidney disease (“CKD”) and vitamin D insufficiency (target March 29, 2016 PDUFA date) and VARUBI™ for chemotherapy-induced nausea and vomiting (launched by partner TESARO in November 2015). Our pharmaceutical business includes OPKO Biologics, which features hGH-CTP, a once-weekly human growth hormone injection (in Phase 3 and partnered with Pfizer), and a longer acting Factor VIIa drug for hemophilia (Phase 2a).
In addition to our pharmaceutical and diagnostic development programs, we own established pharmaceutical platforms in Ireland, Chile, Spain and Mexico which generate revenue and which we expect to facilitate future market entry for our products currently in development. We have a development and commercial supply pharmaceutical company, as well as a global supply chain operation and holding company in Ireland, which we expect will play an important role in the development, manufacturing, distribution and approval of a wide variety of drugs with an emphasis on high potency products. We also own a specialty active pharmaceutical ingredients (“APIs”) manufacturer in Israel, which we expect will facilitate the development of our pipeline of molecules and compounds for our proprietary molecular diagnostic and therapeutic products.
We have a highly experienced management team that we believe has demonstrated an ability to successfully build and manage pharmaceutical and healthcare businesses. Based on their experience in the industry, we believe that our management team has extensive development, regulatory and commercialization expertise and relationships that provide access to commercial opportunities.
All product or service marks appearing in type form different from that of the surrounding text are trademarks or service marks owned, licensed to, promoted or distributed by OPKO, its subsidiaries or affiliates, except as noted. All other trademarks or services marks are those of their respective owners.
GROWTH STRATEGY
We expect our future growth to come from leveraging our commercial infrastructure, proprietary technology and development strengths, and by opportunistically pursuing complementary, accretive, or strategic acquisitions and investments.
We have under development a broad and diversified portfolio of diagnostic tests, vaccines, small molecules, and biologics targeting a broad range of unmet medical needs. We also operate the third largest full service clinical laboratory in the United States. We intend to continue to leverage our proprietary technology and our strengths in all phases of research and development to further develop and commercialize our portfolio of proprietary pharmaceutical and diagnostic products. In support of our strategy, we intend to:
• |
obtain requisite regulatory approval and compile clinical data for our most advanced product candidates; |
• |
develop a focused commercialization capability both internationally and in the U.S.; and |
• |
expand into other medical markets that provide significant opportunities and that we believe are complementary to and synergistic with our business. |
In addition, we expect to leverage the Bio-Reference business and infrastructure to drive rapid and widespread uptake of our diagnostic products, including the 4Kscore test and the Claros 1 in-office immunoassay platform. We also intend to leverage the genetic and genomic data generated and accumulated through Bio-Reference’s genetic sequencing laboratory to enhance drug discovery and clinical trial programs.
We have and expect to continue to be opportunistic and to pursue complementary or strategic acquisitions, licenses and investments. Our management team has significant experience in identifying, executing and integrating these transactions. We expect to use well-timed, carefully selected acquisitions, licenses and investments to continue to drive our growth, including:
5
• |
Products and technologies. We intend to continue to pursue product and technology acquisitions and licenses that will complement our existing businesses and provide new product and market opportunities, enhance our profitability, leverage our existing assets, and contribute to our own organic growth.
|
• |
Commercial businesses. We intend to continue to pursue acquisitions of commercial businesses that will both drive our growth and provide geographically diverse sales and distribution opportunities.
|
• |
Early stage investments. We have and may continue to make investments in early stage companies that we perceive to have valuable proprietary technology and significant potential to create value for OPKO as a shareholder.
|
CORPORATE INFORMATION
We were originally incorporated in Delaware in October 1991 under the name Cytoclonal Pharmaceutics, Inc., which was later changed to eXegenics, Inc. (“eXegenics”). On March 27, 2007, we were part of a three-way merger with Froptix Corporation (“Froptix”) and Acuity Pharmaceuticals, Inc. (“Acuity”), both research and development companies. On June 8, 2007, we changed our name to OPKO Health, Inc. Our shares are publicly traded on the NYSE under the ticker “OPK” and on the Tel Aviv Stock Exchange. Our principal executive offices are located in leased office space in Miami, Florida.
We currently manage our operations in two reportable segments, diagnostics and pharmaceutical. The pharmaceutical segment consists of our pharmaceutical operations we acquired in Chile, Mexico, Ireland, Israel and Spain and our pharmaceutical research and development operations. The diagnostics segment primarily consists of our clinical laboratory operations we acquired through the acquisitions of Bio-Reference and OPKO Lab and our point-of-care operations. There are no significant inter-segment sales. We evaluate the performance of each segment based on operating profit or loss. There is no inter-segment allocation of interest expense and income taxes. Refer to Note 16 for financial information about the segments and geographic areas.
CURRENT PRODUCTS AND SERVICES AND RELATED MARKETS
Diagnostics
Bio-Reference Laboratories
In August 2015, we completed the acquisition of Bio-Reference, the third largest full service clinical laboratory in the United States. Through Bio-Reference, we now offer comprehensive laboratory testing services utilized by healthcare providers in the detection, diagnosis, evaluation, monitoring, and treatment of diseases, including esoteric testing, molecular diagnostics, anatomical pathology, genetics, women’s health and correctional healthcare. We market and sell these services to physician offices, clinics, hospitals, employers and governmental units nationally, with the largest concentration of business in the larger metropolitan areas across New York, New Jersey, Maryland, Pennsylvania, Delaware, Washington DC, Florida, California, Texas, Illinois and Massachusetts. Bio-Reference has a 420-person sales force and operates a network of more than 180 patient service centers for collection of patient specimens.
Our Bio-Reference laboratory testing business consists of routine testing and esoteric testing. Routine tests measure various health parameters, such as the functions of the heart, kidney, liver, thyroid and other organs, including such tests as blood cell counts, cholesterol levels, pregnancy, substance abuse and urinalysis. These tests are primarily performed at our main processing facility in Elmwood Park, New Jersey, as well as satellite facilities in Florida, Texas, Maryland, Ohio, New York and Connecticut. We typically operate 24 hours per day, 365 days per year and perform and report most routine test results within 24 hours.
The esoteric tests we perform require sophisticated equipment and materials, highly skilled personnel and professional attention. Esoteric tests are ordered less frequently than routine tests but typically are priced higher than routine tests. Esoteric tests include tests related to endocrinology, genetics and genomics, immunology, microbiology, HIV tests, molecular diagnostics, oncology, serology, and toxicology. We perform cancer cytogenetic testing at our main processing facility in Elmwood Park, and at our facilities in Clarksburg, MD, and Milford, MA, and genetic testing at our GeneDx facility in Gaithersburg, MD, as well as at our Elmwood Park facility. We perform cytology testing in Frederik, MD, Milford, MA, Columbus, OH, Houston, TX, Melbourne, FL and Campbell, CA, and at our Elmwood Park facility.
Through Bio-Reference, we operate in the following highly specialized laboratory divisions:
• |
Bio-Reference Laboratories. Bio-Reference constitutes our core clinical testing laboratory offering automated, high volume routine testing services, STAT testing, informatics, HIV, Hep C and other molecular tests.
|
6
• |
GenPath (Oncology). National Oncology presence with expertise in cancer pathology and diagnostics, as well as molecular diagnostics. Core tests include FLOW, IHC, MicroArray, FISH, ISH, Morphology, full service oncology.
|
• |
GenPath (Women’s Health). Innovative technology platform for sexually transmitted infections has enabled expansion nationally with specimens coming from 48 contiguous states, including Image Directed Paps, HPV Plus, and STI Testing.
|
• |
GeneDx. Industry leading national laboratory for testing rare and ultra-rare genetic diseases with international reach, performing testings on specimens from more than 50 countries.
|
• |
Laboratorio Bueno Salud. National testing laboratory dedicated to serving the Spanish-speaking population in the United States, where all business is conducted in Spanish including patient and physician interaction.
|
We have one of the largest marketing staffs of any laboratory in the country with sales and marketing groups dedicated to urology, oncology, women’s health, genetic testing and correctional health, as well as cross-over groups selling to large institutions. All of our sales and marketing personnel operate in a dual capacity, as both marketing and client support representatives, which we believe provides better customer service and a strong connection with our customers.
We expect the clinical laboratory testing industry will continue to experience growth in testing volumes due to aging of the population in the U.S., patient awareness of the value of laboratory tests, a decrease in the cost of tests, the development of sophisticated and specialized tests for detection and management of disease, increased recognition of early detection and prevention as a means of reducing healthcare costs, and ongoing research and development in genetics and genomics and personalized medicine. Our mission is to be recognized by our clients as the premier provider of clinical laboratory testing, information and related services.
Bio-Reference provides us a significant diagnostics commercial infrastructure for marketing and sales that reaches more than 10 million patients a year. In addition, its large team of managed care experts complement our efforts to ensure that payors recognize the value of our diagnostic and laboratory tests for reimbursement purposes. Since the acquisition of Bio-Reference, we have begun to leverage the national marketing, sales and distribution resources of Bio-Reference, along with its 420-person sales force, to enhance sales of and reimbursement for our 4Kscore test, a laboratory developed blood test that provides a personalized risk score for aggressive prostate cancer. We plan to continue to leverage the Bio-Reference commercial infrastructure and capabilities, as well as its extensive relationships with payers, to commercialize OPKO’s other diagnostic products under development, including the Claros 1.
4Kscore
We began selling the 4Kscore test in the U.S. in March 2014 and in Europe and Mexico in September 2014 and January 2015, respectively. The 4Kscore test is a laboratory developed test that measures the blood plasma levels of four different prostate-derived kallikrein proteins: Total PSA, Free PSA, Intact PSA and Human Kallikrein-2 (“hK2”). These biomarkers are then combined with a patient’s age, DRE status (nodule / no nodule), and prior negative biopsy status (yes / no) using a proprietary algorithm to calculate the risk (probability) of finding a Gleason Score 7 or higher prostate cancer. The four kallikrein panel of biomarkers utilized in the 4Kscore test is based on decades of research conducted by scientists at Memorial Sloan-Kettering Cancer Center and leading European institutions. Investigators at the University of Malmo, Sweden, University of Turku, Finland and Memorial Sloan Kettering Cancer Center, New York, have also demonstrated that an algorithm integrating these biomarkers along with patient data can predict prostate biopsy results to identify patients with the greatest risk of having aggressive prostate cancer.
The 4Kscore test was developed by OPKO Lab and validated in 2014 in a prospective, blinded study of 1,012 men in collaboration with 26 urology centers across the U.S. Results showed that the 4Kscore test was highly accurate for predicting the presence of high-grade cancer (Gleason score 7 or higher) prior to prostate biopsy. The full data from the blinded, prospective U.S. clinical validation study were presented at the AUA Annual Meeting in Orlando, FL on May 18, 2014 at Plenary Session and published in the online edition of European Urology in October 2014.
The clinical data presented at the AUA annual meeting included 1,012 men scheduled for prostate biopsy. Patients were enrolled regardless of their PSA, age, DRE result, or primary versus repeat biopsy status, and represent contemporary practice in the U.S. The results demonstrated the ability of the 4Kscore test to discriminate between men with high-grade, aggressive prostate cancer and those men who had no findings of cancer or had low-grade or indolent form of the disease. The discrimination, measured by Area Under the Curve (“AUC”) analysis, was 0.82 and was significantly higher than previously developed tests. Furthermore, the 4Kscore test demonstrated excellent risk calibration, indicating the accuracy of the result for an individual patient. The high value of AUC and the excellent risk calibration make the 4Kscore test result valuable information for the shared decision-making between the urologist and patient on whether or not to perform a prostate biopsy.
7
A recent study indicated that the 4Kscore test led to 64.6% fewer biopsies. The study, “The 4Kscore® Test Reduces Prostate Biopsy Rates in Community and Academic Urology Practices”, published in the January 2016 edition of Reviews in Urology, which included 611 patients seen by 35 academic and community urologists across the U.S., evaluated the influence of the 4Kscore test on urologist-patient decisions about whether to perform a biopsy in men who had an abnormal PSA and or DRE result. Test results for patients were stratified into low risk (< 7.5%), intermediate risk (7.5%-19.9%) and high risk (≥20%) for developing aggressive prostate cancer. Nearly half (49.3%) of the men were categorized as low risk; 25.7% and 25.0% fell into the intermediate-risk and high-risk categories, respectively. Notably, the 4Kscore test results influenced biopsy decisions in 88.7% of the men. In the three risk groups, a biopsy was avoided in 94.0%, 52.9%, and 19.0% of men in the low, intermediate, and high-risk categories, respectively.
We have been granted a Category I CPT code by the AMA for our 4Kscore test, which will be published in August 2016 and effective January 1, 2017. This upgrades the 4Kscore test from a Category III Administrative code to a Category I CPT code, a designation reserved for established diagnostic tests. CPT codes are used by insurance companies and government payers to describe health care services and procedures, and having a Category I CPT code is critical to facilitate reimbursement in government programs such as Medicare and Medicaid, as well as private insurance programs. We believe having the Category I CPT code will help facilitate obtaining broader coverage from payers for the 4Kscore test and allow greater access to the test for a broader group of patients across the U.S.
The National Comprehensive Cancer Network (“NCCN”) also included the 4Kscore test as a recommended test in their 2015 Guidelines for Prostate Cancer Early Detection. The panel making this recommendation concluded that the 4Kscore test is indicated for use prior to a first prostate biopsy, or after a negative biopsy, to assist patients and physicians in further defining the probability of high-grade cancer.
As a result of our leveraging the Bio-Reference commercial infrastructure and managed care expertise, together with the NCCN Guidelines publication and receipt of a Category I CPT Code, we expect to significantly expand our efforts to obtain broad reimbursement for the 4Kscore test throughout 2016 and beyond.
Point-of-Care Diagnostics
OPKO Diagnostics, LLC (“OPKO Diagnostics”), formerly Claros Diagnostics, Inc., is developing a novel diagnostic instrument system to provide rapid, high performance blood test results and enable tests to be run in point-of-care settings. The instrument, a microfluidics-based diagnostic test system consisting of a credit card-sized disposable test cassette that works with a small but sophisticated desktop analyzer, provides high performance quantitative blood test results within minutes and permits the transition of complex immunoassays and other tests from the centralized reference laboratory to the physician’s office or hospital nurses station. The technology only requires a finger stick drop of blood introduced into the test cassette which can simultaneously run multiple tests (multiplex) on the single droplet of blood.
We have already obtained a CE Mark for the Claros 1 point-of-care analyzer and a diagnostic test for prostate specific antigen (“PSA”) performed on the Claros 1. We intend to update our CE Mark with all product improvements made to the Claros 1 and Sangia Total PSA test since the initial CE mark approval and introduce the Claros 1 system for PSA in Europe in 2016.
We intend to commence clinical trials and submit our application to the FDA for a pre-marketing authorization (“PMA”) for the PSA test in late 2016 or early 2017. We also intend to submit our application to the FDA for clearance of a testosterone diagnostic test for our point-of-care system in late 2016 or early 2017. We expect to fully leverage Bio-Reference’s marketing, sales and distribution resources for the launch of the Claros 1 system and associated diagnostic tests in the U.S after FDA clearance or approval.
We are also presently working to add additional tests for our point-of-care system, including vitamin D, and we believe that there are many more applications for the technology, including infectious disease, cardiology, women’s health, and companion diagnostics.
Pharmaceutical Business
We presently have several pharmaceutical compounds and technologies in research and development for a broad range of indications and conditions. Our product development candidates are in various stages of development and include the following:
Renal Products
8
Our two lead renal products are Rayaldee (CTAP101), a vitamin D prohormone to treat SHPT in patients with stage 3 or 4 CKD and vitamin D insufficiency, and Alpharen (Fermagate Tablets), a new and potent non-absorbed phosphate binder to treat hyperphosphatemia in Stage 5 patients on chronic hemodialysis. In May 2015, we submitted an NDA for Rayaldee to the FDA. Our NDA was accepted by the FDA for review in July 2015 and the FDA set a PDUFA target date of March 29, 2016. We announced successful top-line results from two pivotal phase 3 trials of Rayaldee in the third quarter of 2014. These trials were identical randomized, double-blind, placebo-controlled, multi-site studies intended to establish the safety and efficacy of Rayaldee as a new treatment for SHPT in patients with stage 3 or 4 CKD and vitamin D insufficiency.
Vitamin D insufficiency arises in CKD due to the abnormal upregulation of CYP24, an enzyme that destroys vitamin D and its metabolites. Studies in CKD patients have demonstrated that currently available over-the-counter and prescription vitamin D products cannot reliably raise blood vitamin D prohormone levels and effectively treat SHPT, a condition commonly associated with CKD in which the parathyroid glands secrete excessive amounts of parathyroid hormone (“PTH”). Prolonged elevation of blood PTH causes excessive calcium and phosphorus to be released from bone, leading to elevated serum calcium and phosphorus levels, softening of the bones (osteomalacia) and calcification of vascular and renal tissues. SHPT affects 40-82% of patients with stage 3 or 4 CKD and approximately 95% of patients with stage 5.
The completed pivotal trials for Rayaldee successfully met all primary efficacy and safety endpoints. The primary efficacy endpoint was a responder analysis in which “responder” was defined as any treated subject who demonstrated an average 30% decrease in PTH from pre-treatment baseline during the last six weeks of the 26-week treatment period. A significantly higher response rate was observed with Rayaldee which steadily increased with treatment duration. The response rate with Rayaldee was similar in CKD stages 3 and 4. Safety and tolerability data were comparable in both treatment groups. Patients completing the two pivotal trials were treated, at their election, for an additional six months with Rayaldee during an open-label extension study.
In addition to SHPT in CKD patients, we also are developing Rayaldee for other indications, and in August 2014, announced the submission of an IND to the FDA to evaluate Rayaldee as an adjunctive therapy for the prevention of skeletal-related events in patients with bone metastases undergoing anti-resorptive therapy. We commenced a phase 1 dose escalation study in the fourth quarter of 2014 in breast and prostate cancer patients with bone metastases who are receiving anti-resorptive therapy. The study is evaluating safety, markers of mineral metabolism and tumor progression.
Our phosphate binder, Alpharen (Fermagate Tablets), has been shown to be safe and effective in treating hyperphosphatemia in phase 2 and 3 trials in stage 5 CKD patients undergoing chronic hemodialysis. Hyperphosphatemia, or elevated serum phosphorus, is common in dialysis patients and tightly linked to the progression of SHPT. The kidneys provide the primary route of excretion for excess phosphorus absorbed from ingested food. As kidney function worsens, serum phosphorus levels increase and directly stimulate PTH secretion. Stage 5 CKD patients must reduce their dietary phosphate intake and usually require regular treatment with phosphate binding agents to lower serum phosphorus to meet the recommendations of the National Kidney Foundation’s Clinical Practice Guidelines that serum phosphorus levels should be maintained at or below 5.5 mg/dL. Hyperphosphatemia contributes to soft tissue mineralization and affects approximately 90% of dialysis patients. Dialysis patients require ongoing phosphate binder treatment to maintain controlled serum phosphorus levels. We are currently preparing a single remaining Phase 3 clinical trial in the U.S., but are first studying novel characteristics of Alpharen which may offer additional competitive advantages.
We believe the CKD patient population is large and growing as a result of obesity, hypertension and diabetes; therefore this patient population represents a significant market opportunity. According to the National Kidney Foundation, CKD afflicts over 26 million people in the U.S., including more than 20 million patients with stage 3 or 4 CKD. In stage 5, kidney function is minimal to absent and patients require regular dialysis or a kidney transplant for survival. An estimated 71-97% of CKD patients have vitamin D insufficiency which can lead to SHPT and its debilitating consequences. CKD continues to be associated with poor outcomes, reflecting the inadequacies of the current standard of care. Vitamin D insufficiency, hyperphosphatemia and SHPT, when inadequately treated, are major contributors to poor CKD outcomes. We intend to develop Rayaldee and Alpharen to constitute part of the foundation for a new and markedly improved standard of care for CKD patients having SHPT and/or hyperphosphatemia.
9
OPKO Biologics
OPKO Biologics is our biopharmaceutical business focused on developing and commercializing longer-acting proprietary versions of already approved therapeutic proteins. One of our innovative platform technologies uses a short, naturally-occurring amino acid sequence (carboxl terminal peptide or “CTP”) that has the effect of slowing the removal from the body of the therapeutic protein to which it is attached. This CTP can be readily attached to a wide array of existing therapeutic proteins, stabilizing the therapeutic protein in the bloodstream and extending its life span without additional toxicity or loss of desired biological activity. We are using the CTP technology to develop new, proprietary versions of certain existing therapeutic proteins that have longer life spans than therapeutic proteins without CTP. We believe that our products will have greatly improved therapeutic profiles and distinct market advantages.
There are two existing biopharmaceuticals on the market that currently utilize CTP technology. The first product is human chorionic gonadotropin (“hCG”), of which CTP is naturally a part. Besides being present normally in high amounts during pregnancy, it is also given therapeutically to women or men as a fertility treatment (sold by Merck-Serono, Merck & Co. and Ferring). The second product is ELONVA® (FSH-CTP), which is sold by Merck & Co. The data from the clinical and therapeutic use of these products gave us confidence that the CTP technology is able to address the major problems faced by the other attempted approaches to increase protein lifespan. Clinical and therapeutic data from these products also reassured us that CTP can be used safely and that it is effective in extending the serum lifetime and activity. We are the exclusive licensee for the utilization of CTP technology in all therapeutic proteins, peptides and their modified forms except for human FSH, LH, TSH and hCG.
Our lead product candidate utilizing CTP, hGH-CTP, is a recombinant human growth hormone product under development for the treatment of growth hormone deficiency (“GHD”), which is a pituitary disorder resulting in short stature in children and other physical ailments in both children and adults.
In December 2014, we entered into an exclusive worldwide agreement with Pfizer for the development and commercialization of hGH-CTP for the treatment of GHD in adults and children, as well as for the treatment of growth failure in children born SGA. In connection with the transaction, we granted Pfizer an exclusive license to commercialize hGH-CTP worldwide, and we received non-refundable and non-creditable upfront payments of $295 million and are eligible to receive up to an additional $275 million upon the achievement of certain regulatory milestones. In addition, we are eligible to receive initial tiered royalty payments associated with the commercialization of hGH-CTP for Adult GHD with percentage rates ranging from the high teens to mid-twenties. Upon the launch of hGH-CTP for Pediatric GHD in certain major markets, the royalties will transition to regional, tiered gross profit sharing for both hGH-CTP and Pfizer’s Genotropin®.
Pursuant to our agreement with Pfizer, we will lead the clinical development activities for the hGH-CTP program and will be responsible for funding the development programs for the key indications, which includes Adult and Pediatric GHD and Pediatric SGA. Pfizer will be responsible for all development costs for additional indications as well as all post-marketing studies. In addition, Pfizer will fund the commercialization activities for all indications and lead the manufacturing activities covered by the global development plan.
GHD occurs when the production of growth hormone, secreted by the pituitary gland, is disrupted. Since growth hormone plays a critical role in stimulating body growth and development, and is involved in the production of muscle protein and in the breakdown of fats, a decrease in the hormone affects numerous body processes. hGH is used for the long-term treatment of children and adults with inadequate secretion of endogenous growth hormone. The primary indications it treats in children are GHD, SGA, kidney disease, Prader-Willi Syndrome and Turner’s Syndrome. In adults, the primary indications are replacement of endogenous growth hormone and the treatment of AIDS-induced weight loss. Patients using hGH receive daily injections six or seven times a week. This is particularly burdensome for pediatric patients. We believe a significant market opportunity exists for a longer-lasting version of hGH that would require fewer injections.
hGH-CTP is currently in a global Phase 3 trial in adults and a global phase 2 trial in children and has orphan drug designation in the U.S. and Europe for both adults and children with GHD. We anticipate commencing our global phase 3 trial in children in the second half of 2016.
In addition to hGH-CTP, we are developing a product to extend the life span of Factor VIIa (hemophilia) using the CTP technology. In February 2013, the FDA granted orphan drug designation to our longer-acting version of clotting Factor VIIa, Factor VIIa-CTP, for the treatment of bleeding episodes in patients with hemophilia A or B with inhibitors to Factor VIII or Factor IX. These patients are currently being treated by commercially-available Factor VIIa, with estimated 2013 worldwide sales of $1.7 billion. Currently, Factor VIIa therapy is available only as an intravenous (IV) formulation which, due to Factor VIIa’s short half-life, requires multiple infusions to treat a bleeding episode. In addition, frequent infusions are onerous when used as preventative prophylactic therapy, especially for children.
10
Pre-clinical studies of IV and subcutaneous formulations of our product in hemophilic animal models demonstrated its duration of action and significantly increased survival. In January 2015, we submitted an IND to the FDA to conduct a Phase 2a study of Factor VIIa-CTP for the treatment of bleeding episodes in hemophilia A or B patients with inhibitors to Factor VIII or Factor IX, which was accepted by the FDA in March 2015. The Phase 2a study commenced in February 2016. Factor VIIa-CTP has been granted orphan designation in Europe as well as the U.S.
We believe that the CTP technology may also be broadly applicable to other best-selling therapeutic proteins in the market and provide several key advantages over our competitor’s existing products: significant reduction in the number of injections required to achieve the same or superior therapeutic effect from the same dosage; faster commercialization with greater chance of success and lower costs than those typically associated with a new therapeutic protein; and manufacturing using industry-standard biotechnology-based protein production processes.
In addition to hGH-CTP and Factor VII-CTP, our internal product development program is currently focused on extending the circulatory half life of oxyntomodulin. Oxyntomodulin, a natural appetite suppressor, is a peptide hormone secreted by the intestine following food intake that induces satiety when it reaches the brain. Oxyntomodulin activates both the glucagon-like peptide-1 receptor (“GLP1R”) and glucagon receptor (“GCGR”) and has been found to decrease food intake and body weight as well as lower glucose in overweight human volunteers.
We believe oxyntomodulin has potential to be a safe, long term therapy for obese and diabetes type II patients, representing significant market opportunities. More than 380 million are living with diabetes worldwide, of which approximately 90% have type II diabetes. According to the World Health Organization, there are more than 500 million severely overweight or obese people.
The clinical utility of oxyntomodulin has been limited mostly because of its short circulating half life. We are developing a long-acting oxyntomodulin comprising oxyntomodulin linked at its N-terminus to a polyethylene glycol (“PEG”) linear chain through a proprietary bi-functional hydrolysable linker. Administration of the conjugate into the blood results in slow release of the non-modified natural oxyntomodulin. Our preclinical studies have shown that a single weekly injection of our compound in development significantly inhibited food intake and reduced body weight in obese and diabetic animal models, as well as improving the lipid profile by reducing cholesterol levels in obese and diabetic mice. We expect to initiate a phase 1 study of oxyntomodulin in the first quarter of 2016.
APIs
FineTech Pharmaceutical, Ltd. (“FineTech”), is our Israeli-based subsidiary that develops and produces high value, high potency specialty APIs. Through its FDA registered facility in Nesher, Israel, FineTech currently manufactures commercial APIs for sale or license to pharmaceutical companies in the U.S., Canada, Europe and Israel. We believe that FineTech’s significant know-how and experience with analytical chemistry and organic syntheses, together with its production capabilities, may play a valuable role in the development of our pipeline of proprietary molecules and compounds for diagnostic and therapeutic products, while providing revenues and profits from its existing API business.
Oligonucleotide Therapeutics
OPKO CURNA, LLC (“CURNA”), previously CURNA Inc., is engaged in the discovery of new drugs for the treatment of a wide variety of illnesses, including cancer, heart disease, metabolic disorders and a range of genetic anomalies. CURNA’s broad platform technology utilizes a short, single strand oligonucleotide and is based on the up-regulation of protein production through interference with non-coding RNA’s, or natural antisense. This strategy contrasts with established approaches which down-regulate protein production. CURNA has designed a novel type of therapeutic modality, termed AntagoNAT, and has initially demonstrated this approach for up-regulation of several therapeutically relevant proteins in in vitro and animal models. We believe that this short, single strand oligonucleotide can be delivered intravenously or subcutaneously without the drug delivery or cell penetration complications typically associated with double stranded siRNA therapeutics. CURNA has identified and developed compounds which increase the production of over 80 key proteins involved in a large number of individual diseases. We have ongoing pre-clinical studies for several of these compounds, with an initial focus on orphan diseases including Dravet Syndrome, Rett Syndrome and MPS-1.
11
NK-1 Program
We acquired rolapitant and other neurokinin-1 (“NK-1”) assets from Merck & Co. In December 2010, we exclusively out-licensed the development, manufacture and commercialization of our lead NK-1 candidate, VARUBI™ (rolapitant), to TESARO. VARUBI™, a potent and selective competitive antagonist of the NK-1 receptor, had successfully completed phase 2 clinical testing for prevention of chemotherapy induced nausea and vomiting, or CINV, and post-operative induced nausea and vomiting. TESARO submitted its NDA to the FDA for approval of oral VARUBI™ in September 2014. TESARO’s NDA for oral VARUBI™ was approved by the FDA in September 2015, and in November 2015, TESARO commenced the commercial launch of VARUBI™ in the United States.
Under the terms of the license, we received a $6.0 million upfront payment from TESARO and are eligible to receive milestone payments of up to $30.0 million upon achievement of certain regulatory and commercial sale milestones (of which $20.0 million has been paid to date) and additional commercial milestone payments of up to $85.0 million if specified levels of annual net sales are achieved. TESARO is also obligated to pay us tiered royalties on annual net sales achieved in the United States and Europe at percentage rates that range from the low double digits to the low twenties, and outside of the United States and Europe at low double-digit percentage rates. TESARO assumed responsibility for clinical development and commercialization of licensed products at its expense. Under the agreement, we will continue to receive royalties on a county-by-country and product-by-product basis until the later of the date that all of the patents rights licensed from us and covering rolapitant expire, are invalidated or are not enforceable, and 12 years from the date of the first commercial sale of the product.
If TESARO elects to develop and commercialize VARUBI™ in Japan through a third-party licensee, TESARO will share equally with us all amounts it receives in connection with such activities, subject to certain exceptions and deductions. In addition, we will have an option to market the products in Latin America. The term of the license will remain in force until the expiration of the royalty term unless we terminate the license earlier for TESARO’s material breach of the license or bankruptcy. TESARO has a right to terminate the license during the term for any reason on three month’s written notice.
Asthma and COPD
In May 2010, we acquired worldwide rights to a novel heparin-derived oligosaccharide which has significant potential in treating asthma and chronic obstructive pulmonary disease (“COPD”). Over 22 million people in the U.S. live with asthma, including nearly 6 million children. Additionally, there are more than 12 million people in the U.S. who have COPD. Currently available therapies often include unwanted side effects and may have limited efficacy. We believe that our product may have an improved efficacy and side effect profile. Our initial studies have demonstrated anti-inflammatory and anti-allergic activity when administered orally or inhaled with inhalers or nebulizers in sheep and mice asthma models. We have also successfully completed human feasibility studies in asthma.
To complement our portfolio of respiratory products, we acquired Inspiro Medical Ltd., a medical device firm developing a new platform to deliver small molecule drugs like corticosteroids and beta agonists or larger molecules to treat respiratory disease. Inspiro’s Inspiromatic is a “smart” easy-to-use dry powder inhaler with several advantages over existing devices. In a First In Man double blinded clinical study conducted in 30 asthmatic children comparing Inspiromatic to a market leading dry powder inhaler, Inspiromatic demonstrated superior pulmonary delivery of the active drug.
Commercial Operations
We also intend to continue to leverage our global commercialization expertise to pursue acquisitions of commercial businesses that will both drive our growth and provide geographically diverse sales and distribution opportunities. During 2015, we acquired EirGen, a growing, profitable and cash flow positive specialty pharmaceutical company based in Ireland. EirGen is focused on the development and commercial supply of high potency, high barrier to entry, pharmaceutical products. Through its facility in Waterford, Ireland, EirGen currently manufactures high potency pharmaceutical products and exports to over 40 countries all over the world. High potency drugs such as those used for cancer chemotherapy are typically unsuitable for manufacture in normal multi-product facilities due to cross contamination risks.
To date, EirGen and its commercial partners have filed 10 product applications with the FDA and 7 in Europe and 5 in Japan. EirGen has a strong research and development portfolio of high barrier to entry drugs and we expect to rapidly expand its drug portfolio. We believe EirGen will play an important role in the development, manufacturing, distribution and approval of a wide variety of drugs in a variety of dosage forms with an emphasis on high potency products.
OPKO Health Europe (previously Farmadiet Group Holding, S.L.) operates primarily in Spain and has more than 20 years of experience in the development, manufacture, marketing, and sale of pharmaceutical, nutraceutical, and veterinary products in Europe.
12
OPKO Mexico (previously Pharmacos Exakta S.A. de C.V.), is engaged in the manufacture, marketing, sale, and distribution of ophthalmic and other pharmaceutical products to private and public customers in Mexico. OPKO Mexico manufacturers and sells products primarily in the generics market in Mexico, although it has recently increased its focus on the development of proprietary products as well.
OPKO Chile (previously Pharma Genexx, S.A.) markets, sells and distributes pharmaceutical and natural products to the private, hospital, pharmacy and public institutional markets in Chile for a wide range of indications, including, cardiovascular products, vaccines, antibiotics, gastro-intestinal products, and hormones, among others. ALS Distribuidora Limitada (“ALS”) is engaged in the business of importation, commercialization and distribution of pharmaceutical products for private markets in Chile. ALS started operations in 2009 as the exclusive product distributor of Arama Laboratorios y Compañía Limitada (“Arama”), a company with more than 20 years of experience in the pharmaceutical products market. In connection with the acquisition of ALS, OPKO acquired all of the product registrations and trademarks previously owned by Arama, as well as the Arama name.
Strategic Investments
We have and may continue to make investments in other early stage companies that we perceive to have valuable proprietary technology and significant potential to create value for OPKO as a shareholder.
RESEARCH AND DEVELOPMENT EXPENSES
During the years ended December 31, 2015, 2014, and 2013, we incurred $99.5 million, $83.6 million, and $53.9 million, respectively, of research and development expenses related to our various product candidates. During the years ended December 31, 2015, 2014 and 2013, our research and development expenses primarily consisted of OPKO Biologics and OPKO Renal development programs including expenses related to the development of hGH-CTP and phase 3 clinical trials for Rayaldee.
INTELLECTUAL PROPERTY
We believe that technology innovation is driving breakthroughs in healthcare. We have adopted a comprehensive intellectual property strategy which blends the efforts to innovate in a focused manner with the efforts of our business development activities to strategically in-license intellectual property rights. We develop, protect, and defend our own intellectual property rights as dictated by the developing competitive environment. We value our intellectual property assets and believe we have benefited from early and insightful efforts at understanding diagnostics, as well as the disease and the molecular basis of potential pharmaceutical intervention.
We actively seek, when appropriate and available, protection for our products and proprietary information by means of U.S. and foreign patents, trademarks, trade secrets, copyrights, and contractual arrangements. Patent protection in the pharmaceutical and diagnostic fields, however, can involve complex legal and factual issues. There can be no assurance that any steps taken to protect such proprietary information will be effective.
We own or license-in over a thousand U.S. and foreign patents and applications for our products, product candidates and our outlicensed product candidates. These patents cover pharmaceuticals, diagnostics and other products and their uses, pharmaceutical and diagnostic compositions and formulations and product manufacturing processes. Our patents are filed in various locations worldwide as is appropriate to the particular patent and its use.
Rayaldee
We have multiple U.S. patent families relating to Rayaldee. These patents are also filed in multiple countries worldwide. One patent family claims a sustained release oral dosage formulation and a method of treating 25-hydroxy vitamin D insufficiency or deficiency and will not expire until at least February 2027. A second patent family claims a method of administering 25-hydroxy vitamin D3 by controlled release, a formulation for controlled release of a vitamin D compound, a controlled release oral dosage formulation of a vitamin D compound and a method of treatment, and will not expire until at least April 2028. We also have additional patent applications pending relating to the sustained release formulation and its use which will expire in 2034 and have licensed patents covering the capsule shell.
Rolapitant
The rolapitant line of patents, licensed to TESARO, includes multiple patent families that cover anti-nausea treatment for chemotherapy patients. These U.S. patents are also filed and granted in many countries around the world. One patent family covers the chemical composition of rolapitant and related compounds and expires in December 2023 (with the patent term
13
adjustment.) A patent term extension request was submitted to the USPTO in October 2015 to obtain an additional 1,716 days which will, upon approval, extend the rolapitant compound patent expiration date to August 2028.The second patent family covers pharmaceutical formulations, including a capsule formulation with a related method of use and expires in April of 2027. The third patent family covers particular aspects of the chemical composition of rolapitant as well as certain methods of treating delayed onset nausea and expires in April 2027. The fourth patent family covers a powdered pharmaceutical composition of a crystalline salt of rolapitant and expires in March 2028. The current line of rolapitant patents are approved for oral treatment. Patent applications directed towards IV formulation of rolapitant are currently pending.
hGH-CTP
The hGH-CTP line of patents, which is currently licensed to Pfizer, Inc., includes two main patent families that cover modified human grown hormone treatment. These U.S. patents are also filed in multiple countries around the world. One patent family covers certain CTP modified hGH polypeptides relating to growth hormones and their method of use and expires in February of 2027 (with the exception of two US patents, namely US 8,304,386 and US 8,097,435, which expire in Jan 2028 and April 2027, respectively, due to Patent Term Adjustment for each). The second patent family covers cytokine-based polypeptides relating to human growth hormone treatment and expires in 2027. In addition to the CTP patents and applications licensed to Pfizer, OPKO has multiple patent families covering similar biologicals with patents and applications pending in the U.S. and internationally.
Because the patent positions of pharmaceutical, biotechnology, and diagnostics companies are highly uncertain and involve complex legal and factual questions, the patents owned and licensed by us, or any future patents, may not prevent other companies from developing similar or therapeutically equivalent products or ensure that others will not be issued patents that may prevent the sale of our products or require licensing and the payment of significant fees or royalties. Furthermore, to the extent that any of our future products or methods are not patentable, that such products or methods infringe upon the patents of third parties, or that our patents or future patents fail to give us an exclusive position in the subject matter claimed by those patents, we will be adversely affected. We may be unable to avoid infringement of third party patents and may have to obtain a license, defend an infringement action, or challenge the validity of the patents in court. A license may be unavailable on terms and conditions acceptable to us, if at all. Patent litigation is costly and time consuming, and we may be unable to prevail in any such patent litigation or devote sufficient resources to even pursue such litigation.
LICENSES AND COLLABORATIVE RELATIONSHIPS
Our strategy is to develop a portfolio of product candidates through a combination of internal development, acquisition, and external partnerships. Collaborations are key to our strategy and we continue to build relationships and forge partnerships in various areas where unmet medical need and commercial opportunities exist. In December 2014, we entered into an exclusive agreement with Pfizer for the development and commercialization of our long-acting hGH-CTP for the treatment of GHD in adults and children, as well as for the treatment of growth failure in children born small for gestational age. Previously, we (or entities we have acquired) have completed strategic licensing transactions with the University of Texas Southwestern Medical Center at Dallas, the President and Fellows of Harvard College, Academia Sinica, The Scripps Research Institute, TESARO, INEOS Healthcare, Arctic Partners, and Washington University, among others.
COMPETITION
The pharmaceutical and diagnostic testing industries are highly competitive and require an ongoing, extensive search for technological innovation. The industries are characterized by rapidly advancing technologies, intense competition and a strong emphasis on proprietary products. They also require, among other things, the ability to effectively discover, develop, test and obtain regulatory approvals for products, as well as the ability to effectively commercialize, market and promote approved products.
Numerous companies, including major pharmaceutical companies, specialty pharmaceutical companies and specialized biotechnology companies, are engaged in the development, manufacture and marketing of pharmaceutical products competitive with those that we intend to commercialize ourselves and through our partners. Competitors to our diagnostics business include major diagnostic companies, reference laboratories, molecular diagnostic firms, universities and research institutions. Most of these companies have substantially greater financial and other resources, larger research and development staffs and more extensive marketing and manufacturing organizations than ours. This enables them, among other things, to make greater research and development investments and efficiently utilize their research and development costs, as well as their marketing and promotion costs, over a broader revenue base. This also provides our competitors with a competitive advantage in connection with the highly competitive product acquisition and product in-licensing process, which may include auctions in which the highest bidder wins. Our competitors may also have more experience and expertise in obtaining marketing approvals from the FDA and other regulatory authorities. In addition to product development, testing, approval, and promotion, other
14
competitive factors in the pharmaceutical and diagnostics industry include industry consolidation, product quality and price, product technology, reputation, customer service, and access to technical information.
In our clinical laboratory operations, we compete with three types of providers in a highly fragmented and competitive industry: hospital laboratories, physician-office laboratories and other independent clinical laboratories. Our major competitors in the New York metropolitan area are two of the largest national laboratories, Quest Diagnostics and Laboratory Corporation of America. Although we are much smaller than these national laboratories, we believe that we compete successfully with them in our region due to our innovative testing services and our level of service. We believe our responses to medical consultation are faster and more personalized than those of the national laboratories. Our client service staff deals only with basic technical questions and those that have medical or scientific significance are referred directly to our senior scientists and medical staff.
We are seeking to commercialize our 4Kscore product in the U.S., Europe and Mexico in a laboratory setting and to capitalize on near-term commercialization opportunities for our proprietary diagnostic point-of-care system by transitioning laboratory-based tests, including the 4Kscore, PSA, testosterone and other tests to our point-of-care system. We expect to leverage Bio-Reference’s national marketing, sales and distribution resources, along with its 420-person sales force to support commercialization of the 4Kscore and Claros 1 products. Competitors to our diagnostics business are many and include major diagnostic companies, molecular diagnostic firms, universities, and research institutions.
Our ability to commercialize our pharmaceutical and diagnostic test product candidates and compete effectively will depend, in large part, on:
• |
our ability to meet all necessary regulatory requirements to advance our product candidates through clinical trials and the regulatory approval process in the U.S. and abroad; |
• |
the perception by physicians and other members of the health care community of the safety, efficacy, and benefits of our products compared to those of competing products or therapies; |
• |
our ability to manufacture products we may develop on a commercial scale; |
• |
the effectiveness of our sales and marketing efforts; |
• |
the willingness of physicians to adopt a new diagnostic or treatment regimen represented by our technology; |
• |
our ability to secure reimbursement for our product candidates; |
• |
the price of the products we may develop and commercialize relative to competing products; |
• |
our ability to accurately forecast and meet demand for our product candidates if regulatory approvals are achieved; |
• |
our ability to develop a commercial scale infrastructure either on our own or with a collaborator, which would include expansion of existing facilities, including our manufacturing facilities, development of a sales and distribution network, and other operational and financial systems necessary to support our increased scale; |
• |
our ability to maintain a proprietary position in our technologies; and |
• |
our ability to rapidly expand the existing information technology infrastructure and configure existing operational, manufacturing, and financial systems (on our own or with third party collaborators) necessary to support our increased scale, which would include existing or additional facilities and or partners. |
15
GOVERNMENT REGULATION
The U.S. government regulates healthcare through various agencies, including but not limited to the following: (i) the FDA, which administers the Federal Food, Drug and Cosmetic Act (“FDCA”), as well as other relevant laws; (ii) the Centers for Medicare & Medicaid Services (“CMS”), which administers the Medicare and Medicaid programs; (iii) the Office of Inspector General (“OIG”), which enforces various laws aimed at curtailing fraudulent or abusive practices, including by way of example, the Anti-Kickback Statute, the Physician Self-Referral Law, commonly referred to as the Stark law, the Anti-Inducement Law, the Civil Money Penalty Law, and the laws that authorize the OIG to exclude healthcare providers and others from participating in federal healthcare programs; and (iv) the Office of Civil Rights, which administers the privacy aspects of the Health Insurance Portability and Accountability Act of 1996. All of the aforementioned are agencies within the Department of Health and Human Services (“HHS”). Healthcare is also provided or regulated, as the case may be, by the Department of Defense through its TriCare program, the Department of Veterans Affairs, especially through the Veterans Health Care Act of 1992, the Public Health Service within HHS under Public Health Service Act § 340B (42 U.S.C. § 256b), the Department of Justice through the Federal False Claims Act and various criminal statutes, and state governments under the Medicaid and other state sponsored or funded programs and their internal laws regulating all healthcare activities.
The testing, manufacture, distribution, advertising, and marketing of drug and diagnostic products and medical devices, as well as the performance of clinical testing services, are subject to extensive regulation by federal, state, and local governmental authorities in the U.S., including the FDA, and by similar agencies in other countries. Any drug, diagnostic, or device product that we develop must receive all relevant regulatory approvals or clearances, as the case may be, before it may be marketed in a particular country.
Clinical Laboratory Operations
Our clinical laboratory operations are subject to regulations, which are designed to ensure the quality and reliability of clinical laboratories by mandating specific standards in the areas of personnel qualifications, administration and participation in proficiency testing, patient test management, quality control, quality assurance and inspections. Laboratories must undergo on-site surveys at least every two years, which may be conducted by the Federal CLIA program or by a private CMS approved accrediting agency. The sanction for failure to comply with CLIA requirements may be suspension, revocation or limitation of a laboratory’s CLIA certificate, which is necessary to conduct business, as well as significant fines and/or criminal penalties. We are also subject to regulation of laboratory operations under state clinical laboratory laws. State clinical laboratory laws may require that laboratories and/or laboratory personnel meet certain qualifications, specify certain quality controls or require maintenance of certain records. Certain states, such as California and Florida, each require that we obtain licenses to test specimens from patients residing in those states and additional states may require similar licenses in the future. Only Washington and New York State are exempt under CLIA, as these states have established laboratory quality standards at least as stringent as CLIA’s. Potential sanctions for violation of these statutes and regulations include significant fines and the suspension or loss of various licenses, certificates and authorizations.
Our clinical laboratory operations are subject to complex laws, regulations and licensure requirements relating to billing and payment for laboratory services, sales and marketing interactions with ordering physicians, security and confidentiality of health information, and environmental and occupational safety, among others. Changes in regulations often increase the cost of testing or processing claims. Also, these laws may be interpreted or applied by a prosecutorial, regulatory or judicial authority in a manner that could require us to make changes in our operations, including in our pricing, billing and/or marketing practices in a manner that could adversely affect operations.
Drug Development
The regulatory process, which includes overseeing preclinical studies and clinical trials of each pharmaceutical compound to establish its safety and efficacy and confirmation by the FDA that good laboratory, clinical, and manufacturing practices were maintained during testing and manufacturing, can take many years, requires the expenditure of substantial resources, and gives larger companies with greater financial resources a competitive advantage over us. Delays or terminations of clinical trials that we undertake would likely impair our development of product candidates. Delays or terminations could result from a number of factors, including stringent enrollment criteria, slow rate of enrollment, size of patient population, having to compete with other clinical trials for eligible patients, geographical considerations, and others.
Although accelerated pathways for approval exist for certain drugs, generally, FDA review processes can be lengthy and unpredictable, and we may encounter delays or rejections of our applications when submitted. Generally, in order to gain FDA approval, we must first conduct preclinical studies in a laboratory and in animal models to obtain preliminary information on a compound and to identify any safety problems. The results of these studies are submitted as part of an IND application that the FDA must review before human clinical trials of an investigational drug can commence.
16
Clinical trials are normally done in three sequential phases and generally take two to five years or longer to complete. Phase 1 consists of testing the drug product in a small number of humans, normally healthy volunteers, to determine preliminary safety and tolerable dose range. Phase 2 usually involves studies in a limited patient population to evaluate the effectiveness of the drug product in humans having the disease or medical condition for which the product is indicated, determine dosage tolerance and optimal dosage, and identify possible common adverse effects and safety risks. Phase 3 consists of additional controlled testing at multiple clinical sites to establish clinical safety and effectiveness in an expanded patient population of geographically dispersed test sites to evaluate the overall benefit-risk relationship for administering the product and to provide an adequate basis for product labeling. Phase 4 clinical trials may be conducted after approval to gain additional experience from the treatment of patients in the intended therapeutic indication.
After completion of clinical trials of a new drug product, FDA and foreign regulatory authority marketing approval must be obtained. Assuming that the clinical data support the product’s safety and effectiveness for its intended use, a NDA is submitted to the FDA for its review. Generally, it takes one to three years to obtain approval. If questions arise during the FDA review process, approval may take a significantly longer period of time. The testing and approval processes require substantial time and effort and we may not receive approval on a timely basis, if at all, or the approval that we receive may be for a narrower indication than we had originally sought, potentially undermining the commercial viability of the product. Even if regulatory approvals are obtained, a marketed product is subject to continual review, and later discovery of previously unknown problems or failure to comply with the applicable regulatory requirements may result in restrictions on the marketing of a product or withdrawal of the product from the market as well as possible civil or criminal sanctions. For marketing outside the U.S., we also will be subject to foreign regulatory requirements governing human clinical trials and marketing approval for pharmaceutical products. The requirements governing the conduct of clinical trials, product licensing, pricing, and reimbursement vary widely from country to country.
None of our pharmaceutical products under development have been approved for marketing in the U.S. or elsewhere. We may not be able to obtain regulatory approval for any such products under development in a timely manner, if at all. Failure to obtain requisite governmental approvals or failure to obtain approvals of the scope requested will delay or preclude us, or our licensees or marketing partners, from marketing our products, or limit the commercial use of our products, and thereby would have a material adverse effect on our business, financial condition, and results of operations. See “Risk Factors — The results of pre-clinical trials and previous clinical trials for our products may not be predictive of future results, and our current and planned clinical trials may not satisfy the requirements of the FDA or other non-U.S. regulatory authorities.”
Device Development
Devices are subject to varying levels of premarket regulatory control, the most comprehensive of which requires that a clinical evaluation be conducted before a device receives approval for commercial distribution. The FDA classifies medical devices into one of three classes: Class I devices are relatively simple and can be manufactured and distributed with general controls; Class II devices are somewhat more complex and require greater scrutiny; Class III devices are new and frequently help sustain life.
In the U.S., a company generally can obtain permission to distribute a new device in one of two ways. The first applies to any device that is substantially equivalent to a device first marketed prior to May 1976, or to another device marketed after that date, but which was substantially equivalent to a pre-May 1976 device. These devices are either Class I or Class II devices. To obtain FDA permission to distribute the device, a company generally must submit a section 510(k) submission, and receive an FDA order finding substantial equivalence to a predicate device (pre-May 1976 or post-May 1976 device that was substantially equivalent to a pre-May 1976 device) and permitting commercial distribution of that device for its intended use. A 510(k) submission must provide information supporting a claim of substantial equivalence to the predicate device. If clinical data from human experience are required to support the 510(k) submission, these data must be gathered in compliance with investigational device exemption (“IDE”), regulations for investigations performed in the U.S. The 510(k) process is normally used for products of the type that the Company proposes distributing. The FDA review process for premarket notifications submitted pursuant to section 510(k) takes, on average, about 90 days, but it can take substantially longer if the FDA has concerns, and there is no guarantee that the FDA will “clear” the device for marketing, in which case the device cannot be distributed in the U.S. There is also no guarantee that the FDA will deem the applicable device subject to the 510(k) process, as opposed to the more time-consuming, resource-intensive and problematic, PMA process described below.
The second, more comprehensive, PMA process, which can take a year or longer, applies to a new device that is not substantially equivalent to a pre-1976 product or that is to be used in supporting or sustaining life or preventing impairment. These devices are normally Class III devices. For example, most implantable devices are subject to the approval process. Two steps of FDA approval are generally required before a company can market a product in the U.S. that is subject to approval, as opposed to clearance. First, a company must comply with IDE regulations in connection with any human clinical investigation of the device. These regulations permit a company to undertake a clinical study of a “non-significant risk” device without
17
formal FDA approval. Prior express FDA approval is required if the device is a significant risk device. Second, the FDA must review the company’s PMA application, which contains, among other things, clinical information acquired under the IDE. The FDA will approve the PMA application if it finds there is reasonable assurance that the device is safe and effective for its intended use. The PMA process takes substantially longer than the 510(k) process and it is conceivable that the FDA would not agree with our assessment that a device that we propose to distribute should be a Class I or Class II device. If that were to occur we would be required to undertake the more complex and costly PMA process. However, for either the 510(k) or the PMA process, the FDA could require us to run clinical trials, which would pose all of the same risks and uncertainties associated with the clinical trials of drugs, described above.
Even when a clinical study has been approved by the FDA or deemed approved, the study is subject to factors beyond a manufacturer’s control, including, but not limited to the fact that the institutional review board at a given clinical site might not approve the study, might decline to renew approval which is required annually, or might suspend or terminate the study before the study has been completed. Also, the interim results of a study may not be satisfactory, leading the sponsor to terminate or suspend the study on its own initiative or the FDA may terminate or suspend the study. There is no assurance that a clinical study at any given site will progress as anticipated; there may be an insufficient number of patients who qualify for the study or who agree to participate in the study or the investigator at the site may have priorities other than the study. Also, there can be no assurance that the clinical study will provide sufficient evidence to assure the FDA that the product is safe and effective, a prerequisite for FDA approval of a PMA, or substantially equivalent in terms of safety and effectiveness to a predicate device, a prerequisite for clearance under 510(k). Even if the FDA approves or clears a device, it may limit its intended uses in such a way that manufacturing and distributing the device may not be commercially feasible. For marketing outside the U.S., we also will be subject to foreign regulatory requirements governing clinical trials and marketing approval for medical devices. The requirements governing the conduct of clinical trials, device clearance/approval, pricing, and reimbursement vary widely from country to country. In addition to the regulatory clearance and approval processes described herein, the FDA periodically issues draft guidance documents designed to provide additional detail on or reform aspects of the 510(k) and PMA clearance and approval processes. To the extent the FDA finalizes and implements these documents, the average 510(k) and PMA submission requirements and review times may change and devices that might previously have been cleared under the 510(k) process may require approval under the PMA process (and vice-versa). Additionally, the Medical User Fee Amendments of 2012 authorized the FDA to collect user fees for the review of certain premarket submissions received on or after October 1, 2012, including 510(k) and PMA applications. These fees are intended to improve the device review process, but it is still too early to assess the actual impact on the industry.
After clearance or approval to market is given, the FDA and foreign regulatory agencies, upon the occurrence of certain events, are authorized under various circumstances to withdraw the clearance or approval or require changes to a device, its manufacturing process or its labeling or additional proof that regulatory requirements have been met.
A manufacturer of a device approved through the PMA is not permitted to make changes to the device, which affects its safety or effectiveness without first submitting a supplement application to its PMA and obtaining FDA approval for that supplement. In some instances, the FDA may require clinical trials to support a supplement application. A manufacturer of a device cleared through the 510(k) process must submit another premarket notification if it intends to make a change or modification in the device that could significantly affect the safety or effectiveness of the device, such as a significant change or modification in design, material, chemical composition, energy source or manufacturing process. Any change in the intended uses of a PMA device or a 510(k) device requires an approval supplement or cleared premarket notification. Exported devices are subject to the regulatory requirements of each country to which the device is exported, as well as certain FDA export requirements.
A company that intends to manufacture medical devices is required to register with the FDA before it begins to manufacture the device for commercial distribution. As a result, we and any entity that manufactures products on our behalf will be subject to periodic inspection by the FDA for compliance with the FDA’s Quality System Regulation requirements and other regulations. In the European Community, we will be required to maintain certain International Organization for Standardization (“ISO”), certifications in order to sell products and we or our manufacturers undergo periodic inspections by notified bodies to obtain and maintain these certifications. These regulations require us or our manufacturers to manufacture products and maintain documents in a prescribed manner with respect to design, manufacturing, testing and control activities. Further, we are required to comply with various FDA and other agency requirements for labeling and promotion. The Medical Device Reporting regulations require that we provide information to the FDA whenever there is evidence to reasonably suggest that a device may have caused or contributed to a death or serious injury or, if a malfunction were to occur, could cause or contribute to a death or serious injury. In addition, the FDA prohibits us from promoting a medical device for unapproved indications.
18
Diagnostic Products
Certain of our diagnostic products in development are subject to regulation by the FDA and similar international health authorities. We have an obligation to adhere to the FDA’s cGMP regulations. Additionally, we are subject to periodic FDA inspections, quality control procedures, and other detailed validation procedures. If the FDA finds deficiencies in the validation of our manufacturing and quality control practices, they may impose restrictions on marketing specific products until corrected.
Regulation by governmental authorities in the U.S. and other countries may be a significant factor in how we develop, test, produce and market our diagnostic test products. Diagnostic tests like ours may not fall squarely within the regulatory approval process for pharmaceutical or device products as described above, and the regulatory pathway is not as clear. Although the FDA regulates in vitro diagnostic devices, some companies have successfully commercialized diagnostic tests for various conditions and disease states without seeking clearance or approval for such tests through a 510(k) or PMA approval process. These tests are known as laboratory developed tests (“LDTs”) and are designed, manufactured, and used within a single laboratory that is certified under the Clinical Laboratory Improvement Amendments of 1988 (“CLIA”). CLIA is a federal law that regulates clinical laboratories that perform testing on specimens derived from humans for the purpose of providing information for diagnostic, preventative or treatment purpose. Such LDT testing is currently under the purview of CMS and state agencies that provide oversight of the safe and effective use of LDTs.
However, the FDA has consistently asserted that it has the regulatory authority to regulate LDTs despite historically exercising enforcement discretion. In furtherance of that position, the FDA issued two draft guidance documents in October 2014: (1) Framework for Regulatory Oversight of Laboratory Developed Tests (the “Framework Guidance”); and (2) FDA Notification and Medical Device Reporting for Laboratory Developed Tests (the “Notification Guidance”). The Framework Guidance outlines the FDA’s plan to adopt over time a risk-based approach to regulating LDTs whereby different classifications of LDTs would be subject to different levels of FDA oversight and enforcement, including, for example, prohibitions on adulteration and misbranding, establishment registration and device listing, premarket notification, banned devices, records and reports, good manufacturing practices, adverse event reporting, premarket review of safety, effectiveness, and clinical validity, and quality system requirements. The Notification Guidance is intended to explain how clinical laboratories should notify the FDA of the LDTs they develop and how to satisfy Medical Device Reporting requirements.
If finalized, the Framework Guidance and the Notification Guidance may have a materially adverse effect on the time, cost, and risk associated with the Company’s development and commercialization of LDTs for the U.S. market, and there can be no assurance that clearances or approvals sought by the Company will be granted and maintained. However, the FDA’s authority to regulate LDTs continues to be challenged, and the timeline and process for finalizing the draft guidance documents is unknown. We will continue to monitor changes to all domestic and international LDT regulatory policy so as to ensure compliance with the current regulatory scheme.
Impact of Regulation
The FDA in the course of enforcing the FDCA may subject a company to various sanctions for violating FDA regulations or provisions of the FDCA, including requiring recalls, issuing Warning Letters, seeking to impose civil money penalties, seizing devices that the agency believes are non-compliant, seeking to enjoin distribution of a specific type of device or other product, seeking to revoke a clearance or approval, seeking disgorgement of profits and seeking to criminally prosecute a company and its officers and other responsible parties.
The levels of revenues and profitability of biopharmaceutical companies may be affected by the continuing efforts of government and third party payers to contain or reduce the costs of health care through various means. For example, in certain foreign markets, pricing or profitability of therapeutic and other pharmaceutical products is subject to governmental control. In the U.S., there have been, and we expect that there will continue to be, a number of federal and state proposals to implement similar governmental control. In addition, in the U.S. and elsewhere, sales of therapeutic and other pharmaceutical products are dependent in part on the availability and adequacy of reimbursement from third party payers, such as the government or private insurance plans. Third party payers are increasingly challenging established prices, and new products that are more expensive than existing treatments may have difficulty finding ready acceptance unless there is a clear therapeutic benefit. On April 1, 2014, the Protecting Access to Medicare Act of 2014 (“PAMA”) was enacted into law. Under PAMA, Medicare payment for clinical diagnostic laboratory tests will be established by calculating a weighted mean of private payer rates starting in 2017. Further, applicable laboratories will be required to report payment rates for covered tests starting in 2016. Failure to report such data may result in a civil money penalty in an amount of up to $10,000 per day. It is anticipated that the market-based payment system will result in lower reimbursement rates for clinical diagnostic laboratory tests. Even though the permitted annual decrease will be capped through 2022, the cap does not apply to new tests or new advanced diagnostic tests. We cannot assure you that any of our products will be considered cost effective, or that reimbursement will be available or sufficient to allow us to sell them competitively and profitably.
19
State and Federal Security and Privacy Regulations
The privacy and security regulations under the Health Insurance Portability and Accountability Act of 1996, as amended by the Health Information Technology for Economic and Clinical Health Act of 2009 ( the “HITECH Act”, and collectively, “HIPAA”), establish comprehensive federal standards with respect to the uses and disclosures of protected health information, or PHI, by health plans and health care providers, in addition to setting standards to protect the confidentiality, integrity and availability of electronic PHI. The regulations establish a complex regulatory framework on a variety of subjects, including:
• |
the circumstances under which uses and disclosures of PHI are permitted or required without a specific authorization by the patient, including but not limited to treatment purposes, to obtain payments for services and health care operations activities; |
• |
a patient’s rights to access, amend and receive an accounting of certain disclosures of PHI; |
• |
the content of notices of privacy practices for PHI; and |
• |
administrative, technical and physical safeguards required of entities that use or receive PHI electronically. |
The final “omnibus” rule implementing the HITECH Act took effect on March 26, 2013. The rule is broad in scope, but certain provisions are particularly significant in light of our business operations. For example, the final “omnibus” rule implementing the HITECH Act:
• |
Makes clear that situations involving impermissible access, acquisition, use or disclosure of protected health information are now presumed to be a breach unless the covered entity or business associate is able to demonstrate that there is a low probability that the information has been compromised; |
• |
Defines the term “business associate” to include subcontractors and agents that receive, create, maintain or transmit protected health information on behalf of the business associate; |
• |
Establishes new parameters for covered entities and business associates on uses and disclosures of PHI for fundraising and marketing; and |
• |
Establishes clear restrictions on the sale of PHI without patient authorization. |
As a provider of clinical laboratory services and as we launch commercial diagnostic tests, we must continue to implement policies and procedures related to compliance with the HIPAA privacy and security regulations, as required by law. The privacy and security regulations provide for significant fines and other penalties for wrongful use or disclosure of PHI, including potential civil and criminal fines and penalties.
Anti-Kickback Laws, Physician Self-Referral Laws, False Claims Act, Civil Monetary Penalties
We are also subject to various federal, state, and international laws pertaining to health care “fraud and abuse,” including anti-kickback laws and false claims laws. The federal Anti-Kickback Statute prohibits anyone from knowingly and willfully soliciting, receiving, offering, or paying any remuneration with the intent to refer, or to arrange for the referral or order of, services or items payable under a federal health care program, including the purchase or prescription of a particular drug or the use of a service or device. Recognizing that the Anti-Kickback Statute is broad and may technically prohibit many innocuous or beneficial arrangements, Congress authorized the U.S. Department of Health and Human Services Office of Inspector General, or OIG, to issue a series of regulations, known as “safe harbors.” These safe harbors set forth requirements that, if met in their entirety, will assure health care providers and other parties that they will not be prosecuted under the Anti-Kickback Statute. The failure of a transaction or arrangement to fit precisely within one or more safe harbors does not necessarily mean that it is illegal, or that prosecution will be pursued. However, conduct and business arrangements that do not fully satisfy each applicable safe harbor may result in increased scrutiny by government enforcement authorities, such as the OIG.
Violations of the Anti-Kickback Statute are punishable by the imposition of criminal fines, civil money penalties, treble damages, and/or exclusion from participation in federal health care programs. Many states have also enacted similar anti-kickback laws. The Anti-Kickback Statute and similar state laws and regulations are expansive. If the government were to allege against or convict us of violating these laws, there could be a material adverse effect on our business, results of operations, financial condition, and our stock price. Even an unsuccessful challenge could cause adverse publicity and be costly to respond to, which could have a materially adverse effect on our business, results of operations and financial condition. We will consult counsel concerning the potential application of these and other laws to our business and our sales, marketing and other activities and will make good faith efforts to comply with them. However, given the broad reach of federal and state anti-kickback laws and the increasing attention given by law enforcement authorities, we are unable to predict whether any of our activities will be challenged or deemed to violate these laws.
20
We are also subject to the physician self-referral laws, commonly referred to as the Stark law, which is a strict liability statute that generally prohibits physicians from referring Medicare patients to providers of “designated health services,” including clinical laboratories, with whom the physician or the physician’s immediate family member has an ownership interest or compensation arrangement, unless an applicable exception applies. Moreover, many states have adopted or are considering adopting similar laws, some of which extend beyond the scope of the Stark law to prohibit the payment or receipt of remuneration for the prohibited referral of patients for designated healthcare services and physician self-referrals, regardless of the source of the payment for the patient’s care. If it is determined that certain of our practices or operations violate the Stark law or similar statutes, we could become subject to civil and criminal penalties, including exclusion from the Medicare programs and loss of government reimbursement. The imposition of any such penalties could harm our business.
Another development affecting the health care industry is the increased use of the federal civil False Claims Act and, in particular, actions brought pursuant to the False Claims Act’s “whistleblower” or “qui tam” provisions. The False Claims Act, as amended by the Fraud Enforcement and Recovery Act of 2009 and the Patient Protection and Affordable Care Act of 2010, imposes liability on any person or entity who, among other things, knowingly presents, or causes to be presented, a false or fraudulent claim for payment by a federal health care program. We submit claims for services performed at our laboratories. The qui tam provisions of the False Claims Act allow a private individual to bring actions on behalf of the federal government alleging that the defendant has submitted a false claim to the federal government, and to share in any monetary recovery. In recent years, the number of suits brought by private individuals has increased dramatically. In addition, various states have enacted false claim laws analogous to the False Claims Act. Many of these state laws apply where a claim is submitted to any third-party payor and not merely a federal health care program. When an entity is determined to have violated the False Claims Act, it may be required to pay up to three times the actual damages sustained by the government, plus civil penalties for each separate false claim. There are many potential bases for liability under the False Claims Act. Liability arises, primarily, when an entity knowingly submits, or causes another to submit, a false claim for reimbursement to the federal government. The False Claims Act has been used to assert liability on the basis of inadequate care, kickbacks and other improper referrals, improper use of Medicare numbers when detailing the provider of services, and allegations as to misrepresentations with respect to the services rendered. Our activities relating to the sale and marketing of our products may be subject to scrutiny under these laws. We are unable to predict whether we would be subject to actions under the False Claims Act or a similar state law, or the impact of such actions. However, the costs of defending such claims, as well as any sanctions imposed, could significantly adversely affect our financial performance.
Further, federal law prohibits any entity from offering or transferring to a Medicare or Medicaid beneficiary any remuneration that the entity knows or should know is likely to influence the beneficiary’s selection of a particular provider, practitioner or supplier of Medicare or Medicaid payable items or services, including waivers of copayments and deductible amounts (or any part thereof) and transfers of items or services for free or for other than fair market value. Entities found in violation may be liable for civil monetary penalties of up to $10,000 for each wrongful act. Although we believe that our sales and marketing practices are in material compliance with all applicable federal and state laws and regulations, relevant regulatory authorities may disagree and violation of these laws, or, our exclusion from such programs as Medicaid and other governmental programs as a result of a violation of such laws, could have a material adverse effect on our business, results of operations, financial condition and cash flows.
Foreign Corrupt Practices Act
We are also subject to the U.S. Foreign Corrupt Practices Act (“FCPA”), which prohibits corporations and individuals from paying, offering to pay, or authorizing the payment of anything of value to any foreign government official, government staff member, political party, or political candidate in an attempt to obtain or retain business or to otherwise influence a person working in an official capacity. The FCPA also requires public companies to make and keep books and records that accurately and fairly reflect their transactions and to devise and maintain an adequate system of internal accounting controls. Our international activities create the risk of unauthorized payments or offers of payments by our employees, consultants, sales agents or distributors, even though they may not always be subject to our control. We discourage these practices by our employees and agents. However, our existing safeguards and any future improvements may prove to be less than effective, and our employees, consultants, sales agents or distributors may engage in conduct for which we might be held responsible. Any failure by us to adopt appropriate compliance procedures and ensure that our employees and agents comply with the FCPA and applicable laws and regulations in foreign jurisdictions could result in substantial penalties or restrictions on our ability to conduct business in certain foreign jurisdictions.
21
MANUFACTURING AND QUALITY
Other than our facilities in Waterford, Ireland, Guadalajara, Mexico, Nesher, Israel, and Banyoles, Spain, we currently have no pharmaceutical manufacturing facilities. We have entered into agreements with various third parties for the formulation and manufacture of our pharmaceutical clinical supplies. These suppliers and their manufacturing facilities must comply with FDA regulations, current good laboratory practices (“cGLPs”) and current good manufacturing practices (“cGMPs”). We plan to outsource the manufacturing and formulation of our clinical supplies.
The FDA and similar regulatory bodies may inspect our facilities and the facilities of those who manufacture on our behalf worldwide. If the FDA or similar regulatory bodies inspecting our facilities or the facilities of our suppliers find regulatory violations in manufacturing and quality control practices or procedures they may require us to cease partial or complete manufacturing operations until the violations are corrected. They may also impose restrictions on distribution of specific products until the violations are corrected.
Our point-of-care diagnostic system consists of a disposable test cassette and an analyzer. We prepare all necessary test reagents and assemble and package the disposable cassettes at our facility in Woburn, Massachusetts. We rely on third parties for the manufacture of the analyzer.
We are committed to providing high quality products to our customers, and we plan to meet this commitment by working diligently to continue implementing updated and improved quality systems and concepts throughout our organization.
SALES & MARKETING
Our diagnostics business includes Bio-Reference’s 420-person sales force in the U.S. to drive growth and leverage new products, including the 4Kscore prostate cancer test and the Claros 1 in-office immunoassay platform. We currently do not have pharmaceutical sales or marketing personnel in the U.S., and we have limited personnel in Ireland, Chile, Spain, Mexico and Israel. In order to commercialize any pharmaceutical products that are approved for commercial sale, we must either build a sales and marketing infrastructure or collaborate with third parties with sales and marketing experience.
EMPLOYEES
As of December 31, 2015, we had 5,936 full-time employees worldwide. None of our employees are represented by a collective bargaining agreement.
Code of Ethics
We have adopted a Code of Business Conduct and Ethics. We require all employees, including our principal executive officer and principal accounting officer and other senior officers and our employee directors, to read and to adhere to the Code of Business Conduct and Ethics in discharging their work-related responsibilities. Employees are required to report any conduct that they believe in good faith to be an actual or apparent violation of the Code of Business Conduct and Ethics. The Code of Business Conduct and Ethics is available on our website at http://www.OPKO.com.
Available Information
We make available free of charge on or through our web site, at www.opko.com, our Annual Reports on Form 10-K, Quarterly Reports on Form 10-Q, Current Reports on Form 8-K and all amendments to those reports as soon as reasonably practicable after such material is electronically filed with the SEC. Additionally, the public may read and copy any materials we file with the SEC at the SEC’s Public Reference Room at 100 F Street, NE, Room 1580, Washington, D.C., 20549. Information regarding operation of the Public Reference Room is available by calling the SEC at 1-800-SEC-0330. Information that we file with the SEC is also available at the SEC’s Web-site at www.sec.gov.
ITEM 1A. RISK FACTORS.
You should carefully consider the risks described below, as well as other information contained in this report, including the consolidated financial statements and the notes thereto and “Management’s Discussion and Analysis of Financial Condition and Results of Operations.” The occurrence of any of the events discussed below could significantly and adversely affect our business, prospects, results of operations, financial condition, and cash flows.
RISKS RELATED TO OUR BUSINESS
We have a history of operating losses and may not become profitable in the near future.
22
We are not profitable and have incurred losses since our inception. We do not anticipate that we will generate revenue from the sale of proprietary pharmaceutical products or certain of our diagnostic products for some time and we have generated only limited revenue from our pharmaceutical operations in Chile, Mexico, Israel, Spain, and Ireland, and from sale of the 4Kscore test. Although we expect to leverage the national marketing, sales and distribution resources of Bio-Reference to enhance sales of, and reimbursement for, our 4Kscore test and our other diagnostic products under development, we may not be successful in our integration of Bio-Reference which would adversely impact our ability to generate substantial revenue from the sale of these products for some time. We do not currently have rights to any pharmaceutical product candidates that have been approved for marketing, other than those products sold by our Chilean, Mexican, Israeli, Spanish, and Irish subsidiaries. We continue to incur substantial research and development and general and administrative expenses related to our operations and, to date, we have devoted most of our financial resources to research and development, including our pre-clinical development activities and clinical trials. We may incur losses from our operations for the foreseeable future and these losses could increase as we continue our research activities and conduct development of, and seek regulatory approvals and clearances for, our product candidates, and prepare for and begin to commercialize any approved or cleared products, particularly if we are unable to generate profits and cash flow from Bio‑Reference and our other commercial businesses. If we are unable to generate profits and cash flow from Bio-Reference and our other commercial businesses, our product candidates fail in clinical trials or do not gain regulatory approval or clearance, or if our product candidates do not achieve market acceptance, we may never become profitable. In addition, if we are required by the U.S. Food and Drug Administration (“FDA”), to perform studies in addition to those we currently anticipate, our expenses will increase beyond current expectations and the timing of any potential product approval may be delayed. Even if we achieve profitability in the future, we may not be able to sustain profitability in subsequent periods.
We may require substantial additional funding, which may not be available to us on acceptable terms, or at all.
As of December 31, 2015, we have cash and cash equivalents of $193.6 million. We believe we have sufficient cash and cash equivalents on hand or available to us from operations or through lines of credit to meet our anticipated cash requirements for operations and debt service beyond the next 12 months. We have based this estimate on assumptions that may prove to be wrong or subject to change, and we may be required to use our available capital resources sooner than we currently expect or curtail aspects of our operations in order to preserve our capital. Because of the numerous risks and uncertainties associated with the development and commercialization of our product candidates, the success of our relationship with Pfizer and the success of our acquisition of Bio-Reference, we are unable to estimate the amounts of increased capital outlays and operating expenditures associated with our current and anticipated clinical trials and our expanded commercial operations. Our future capital requirements will depend on a number of factors, including our relationship with Pfizer, the success of the Bio-Reference acquisition and costs associated with the integration of the Bio-Reference operations, the continued progress of our research and development of product candidates, the timing and outcome of clinical trials and regulatory approvals, the costs involved in preparing, filing, prosecuting, maintaining, defending, and enforcing patent claims and other intellectual property rights, the status of competitive products, the availability of financing, and our success in developing markets for our product candidates.
Until we can generate a sufficient amount of product and service revenue to finance our cash requirements for research, development and operations, we will need to finance future cash needs primarily through public or private equity offerings, debt financings, or strategic collaborations. Our ability to obtain additional capital may depend on prevailing economic conditions and financial, business and other factors beyond our control. Disruptions in the U.S. and global financial markets may adversely impact the availability and cost of credit, as well as our ability to raise money in the capital markets. Economic conditions have been, and continue to be, volatile. Continued instability in these market conditions may limit our ability to replace, in a timely manner, maturing liabilities and access the capital necessary to fund and grow our business. There can be no assurance that additional capital will be available to us on acceptable terms, or at all, which could adversely impact our business, results of operations, liquidity, capital resources and financial condition. If we are not able to secure additional funding when needed, we may have to delay, reduce the scope of, or eliminate one or more of our clinical trials or research and development programs. To the extent that we raise additional funds by issuing equity securities, our stockholders may experience additional significant dilution, and debt financing, if available, may involve restrictive covenants. To the extent that we raise additional funds through collaboration and licensing arrangements, it may be necessary to relinquish some rights to our technologies or our product candidates or grant licenses on terms that may not be favorable to us. We may seek to access the public or private capital markets whenever conditions are favorable, even if we do not have an immediate need for additional capital at that time.
Our research and development activities may not result in commercially viable products.
Many of our product candidates are in the early stages of development and are prone to the risks of failure inherent in drug, diagnostic, and medical device product development. These risks further include the possibility that such products would:
23
• |
be found to be ineffective, unreliable, or otherwise inadequate or otherwise fail to receive regulatory approval; |
• |
be difficult or impossible to manufacture on a commercial scale; |
• |
be uneconomical to market or otherwise not be effectively marketed; |
• |
fail to be successfully commercialized if adequate reimbursement from government health administration authorities, private health insurers, and other organizations for the costs of these products is unavailable; |
• |
be impossible to commercialize because they infringe on the proprietary rights of others or compete with products marketed by others that are superior; or |
• |
fail to be commercialized prior to the successful marketing of similar products by competitors. |
The results of pre-clinical trials and previous clinical trials for our products may not be predictive of future results, and our current and planned clinical trials may not satisfy the requirements of the FDA or other non-U.S. regulatory authorities.
Positive results from pre-clinical studies and early clinical trial experience should not be relied upon as evidence that later-stage or large-scale clinical trials will succeed. Likewise, there can be no assurance that the results of studies conducted by collaborators or other third parties will be viewed favorably or are indicative of our own future study results. We may be required to demonstrate with substantial evidence through well-controlled clinical trials that our product candidates are either (i) with respect to drugs or Class III devices, safe and effective for use in a diverse population of their intended uses or (ii) with respect to Class I or Class II devices, are substantially equivalent in terms of safety and effectiveness to devices that are already marketed under section 510(k) of the Food, Drug and Cosmetic Act. Success in early clinical trials does not mean that future clinical trials will be successful because product candidates in later-stage clinical trials may fail to demonstrate sufficient safety and efficacy to the satisfaction of the FDA and other non-U.S. regulatory authorities despite having progressed through initial clinical trials.
Further, our drug candidates may not be approved or cleared even if they achieve their primary endpoints in phase 3 clinical trials or registration trials. In addition our diagnostic test candidates may not be approved or cleared, as the case may be, even though clinical or other data are, in our view, adequate to support an approval or clearance. The FDA or other non-regulatory authorities may disagree with our trial design and our interpretation of data from pre-clinical studies and clinical trials. In addition, any of these regulatory authorities may change requirements for the approval or clearance of a product candidate even after reviewing and providing comment on a protocol for a pivotal clinical trial that has the potential to result in FDA and other non-U.S. regulatory authorities’ approval. Any of these regulatory authorities may also approve or clear a product candidate for fewer or more limited indications or uses than we request or may grant approval or clearance contingent on the performance of costly post-marketing clinical trials. The FDA or other non-U.S. regulatory authorities may not approve the labeling claims necessary or desirable for the successful commercialization of our product candidates.
The results of our clinical trials may show that our product candidates may cause undesirable side effects, which could interrupt, delay or halt clinical trials, resulting in the denial of regulatory approval by the FDA and other non-U.S. regulatory authorities.
In light of widely publicized events concerning the safety risk of certain drug products, regulatory authorities, members of Congress, the Government Accounting Office, medical professionals, and the general public have raised concerns about potential drug safety issues. These events have resulted in the withdrawal of drug products, revisions to drug labeling that further limit use of the drug products, and establishment of risk management programs that may, for instance, restrict distribution of drug products. The increased attention to drug safety issues may result in a more cautious approach by the FDA to clinical trials. Data from clinical trials may receive greater scrutiny with respect to safety, which may make the FDA or other regulatory authorities more likely to terminate clinical trials before completion, or require longer or additional clinical trials that may result in substantial additional expense and a delay or failure in obtaining approval or approval for a more limited indication than originally sought.
The failure to obtain approval for or successfully commercialize Rayaldee would have a material adverse effect on our business.
The NDA for Rayaldee is currently pending before the FDA with a PDUFA target date of March 28, 2016. Upon approval, we expect to begin the commercial launch of Rayaldee in the second half of 2016. There can be no assurance that we will obtain regulatory approval or be able to launch Rayaldee by such dates. Further even if we obtain regulatory approval of Rayaldee, there can be no assurance that we will be able to successfully commercialize Rayaldee. To successfully launch and commercialize Rayaldee, we will need to establish a sales and marketing and clinical support infrastructure, educate the medical community about Rayaldee’s benefits, and establish commercially viable pricing and obtain adequate reimbursement
24
from third-party and government payors. Our failure to successfully commercialize Rayaldee within the expected time frame, or at all, would have a material adverse effect on our business.
Our exclusive worldwide agreement with Pfizer Inc. is important to our business. If we do not successfully develop hGH- CTP and/or Pfizer Inc. does not successfully commercialize hGH-CTP, our business could be adversely affected.
In December 2014, we entered into a development and commercialization agreement with Pfizer relating to our long-acting hGH- CTP for the treatment of growth hormone deficiency in adults and children. Under the terms of the agreements with Pfizer, we received non-refundable and non-creditable upfront payments of $295 million and are eligible to receive up to an additional $275 million upon the achievement of certain regulatory milestones. In addition, we are eligible to receive initial royalty payments associated with the commercialization of hGH-CTP for Adult GHD. Upon the launch of hGH-CTP for Pediatric GHD, the royalties will transition to a regional, tiered gross profit sharing for both hGH-CTP and Pfizer’s Genotropin®. We are also responsible for the development program and are obligated to pay for the development up to an agreed cap, which may be exceeded under certain circumstances. If we are required to exceed the agreed cap, it could have a material adverse impact on the expected benefits to us from the Pfizer transaction and our overall financial condition. In the event that the parties are able to obtain regulatory approvals to market a product covered by the agreement, we will be substantially dependent on Pfizer for the successful commercialization of such product. The success of the collaboration arrangement with Pfizer is dependent in part on, among other things, the skills, experience and efforts of Pfizer’s employees responsible for the project, Pfizer’s commitment to the arrangement, and the financial condition of Pfizer, all of which are beyond our control. In the event that Pfizer, for any reason, including but not limited to early termination of the agreement, fails to devote sufficient resources to successfully develop and commercialize any product resulting from the collaboration arrangement, our ability to earn milestone payments or receive royalty or profit sharing payments would be adversely affected, which would have a material adverse effect on our financial condition and prospects.
Our business is substantially dependent on the success of phase 3 clinical trials for hGH-CTP and our ability to achieve regulatory approval for the marketing of this product.
There is no assurance that phase 3 trials for hGH-CTP will continue to be successful or support marketing approval, or that we will be able to obtain marketing approval for the product, or any other product candidate we are developing. Before they can be marketed, our products in development must be approved by the FDA or similar foreign governmental agencies. The process for obtaining FDA approval is both time-consuming and costly, with no certainty of a successful outcome. Before obtaining regulatory approval for the sale of any drug candidate, we must conduct extensive preclinical tests and clinical trials to demonstrate the safety and efficacy in humans of our product candidates. Although hGH-CTP has exhibited no serious adverse events associated with the drug administration in the clinical trials conducted to date, further testing or patient use may undermine those determinations or unexpected side effects may arise. A failure of any preclinical study or clinical trial can occur at any stage of testing. The results of preclinical and initial clinical testing of these products may not necessarily indicate the results that will be obtained from later or more extensive testing. It also is possible to suffer significant setbacks in advanced clinical trials, even after obtaining promising results in earlier trials. If phase 3 clinical trials for hGH-CTP are not successful or we are unable to achieve regulatory approval for this product, our business will be significantly adversely impacted, which could have a materially adverse effect on our business, financial condition and results of operations.
Our business is substantially dependent on our ability to develop, launch and generate revenue from our diagnostic products.
Our business is dependent on our ability to successfully commercialize the 4Kscore test and other diagnostic products, including the Claros 1. We are committing significant resources to the development and commercialization of these products, and there is no guarantee that we will be able to successfully commercialize these tests. We have limited experience in developing, manufacturing, selling, marketing or distributing diagnostic tests. Although we expect to leverage the national marketing, sales and distribution resources of Bio-Reference to enhance sale of, and reimbursement for, the 4Kscore test and other diagnostic products including the Claros 1, we may not be successful in our integration with Bio-Reference or be able to successfully commercialize our diagnostic products utilizing the Bio-Reference infrastructure. If we are not able to successfully develop, market or sell diagnostic tests we develop for any reason, including the failure to obtain any required regulatory approvals, obtain reimbursement for, or successfully integrate Bio-Reference, we will not generate any meaningful revenue from the sale of such tests. Even if we are able to develop effective diagnostic tests for sale in the marketplace, a number of factors could impact our ability to sell such tests or generate any significant revenue from the sale of such tests, including without limitation:
▪ |
our ability to establish and maintain adequate infrastructure to support the commercial launch and sale of our diagnostic tests, including establishing adequate laboratory space, information technology infrastructure, sample collection and tracking systems, electronic ordering and reporting systems and other infrastructure and hiring adequate laboratory and other personnel; |
25
▪ |
the success of the validation studies for our diagnostic tests under development and our ability to publish study results in peer-reviewed journals; |
▪ |
the availability of alternative and competing tests or products and technological innovations or other advances in medicine that cause our technologies to be less competitive; |
▪ |
the accuracy rates of such tests, including rates of false-negatives and/or false-positives; |
▪ |
concerns regarding the safety or effectiveness or clinical utility of our diagnostic tests; |
▪ |
changes in the regulatory environment affecting health care and health care providers, including changes in laws regulating laboratory testing and/or device manufacturers; |
▪ |
the extent and success of our sales and marketing efforts and ability to drive adoption of our diagnostic tests; |
▪ |
coverage and reimbursement levels by government payors and private insurers; |
▪ |
pricing pressures and changes in third-party payor reimbursement policies; and |
▪ |
intellectual property rights held by others or others infringing our intellectual property rights. |
Our business is substantially dependent on our ability to generate profits and cash flow from our laboratory operations.
We have made a significant investment in our laboratory operations through the acquisitions of OPKO Lab and Bio-Reference. We compete in the clinical laboratory market primarily on the basis of the quality of testing, reporting and information systems, reputation in the medical community, the pricing of services and ability to employ qualified personnel. Our failure to successfully compete on any of these factors could result in the loss of clients and a reduction in our revenues and profits. To offset efforts by payors to reduce the cost and utilization of clinical laboratory services, we will need to obtain and retain new clients and business partners and grow the laboratory operations. A reduction in tests ordered or specimens submitted by existing clients, without offsetting growth in our client base, could impact our ability to successfully grow our business and could have a material adverse impact on our ability to generate profits and cash flow from the laboratory operations.
Discontinuation or recalls of existing testing products, failure to develop, or acquire, licenses for new or improved testing technologies; or our clients using new technologies to perform their own tests could adversely affect our business.
From time to time, manufacturers discontinue or recall reagents, test kits or instruments used by us to perform laboratory testing. Such discontinuations or recalls could adversely affect our costs, testing volume and revenue.
The clinical laboratory industry is subject to changing technology and new product introductions. Our success in maintaining a leadership position in genomic and other advanced testing technologies will depend, in part, on our ability to develop, acquire or license new and improved technologies on favorable terms and to obtain appropriate coverage and reimbursement for these technologies. We may not be able to negotiate acceptable licensing arrangements and it cannot be certain that such arrangements will yield commercially successful diagnostic tests. If we are unable to license these testing methods at competitive rates, our research and development costs may increase as a result. In addition, if we are unable to license new or improved technologies to expand our esoteric testing operations, our testing methods may become outdated when compared with our competition and testing volume and revenue may be materially and adversely affected.
Currently, most clinical laboratory testing is categorized as “high” or “moderate” complexity, and thereby is subject to extensive and costly regulation under CLIA. The cost of compliance with CLIA makes it impractical for most physicians to operate clinical laboratories in their offices, and other laws limit the ability of physicians to have ownership in a laboratory and to refer tests to such a laboratory. Manufacturers of laboratory equipment and test kits could seek to increase their sales by marketing point-of-care laboratory equipment to physicians and by selling test kits approved for home or physician office use to both physicians and patients. Diagnostic tests approved for home use are automatically deemed to be “waived” tests under CLIA and may be performed in physician office laboratories as well as by patients in their homes with minimal regulatory oversight. Other tests meeting certain FDA criteria also may be classified as “waived” for CLIA purposes. The FDA has regulatory responsibility over instruments, test kits, reagents and other devices used by clinical laboratories and has taken responsibility from the Centers for Disease Control for classifying the complexity of tests for CLIA purposes. Increased approval of “waived” test kits could lead to increased testing by physicians in their offices or by patients at home, which could affect our market for laboratory testing services and negatively impact our revenues. If our competitors develop and market products that are more effective, safer or less expensive than our current diagnostic products and our future product candidates, our net revenues, profitability and commercial opportunities will be negatively impacted.
If our competitors develop and market products or services that are more effective, safer or less expensive than our current and future products or services, our revenues, profitability and commercial opportunities will be negatively impacted.
26
The pharmaceutical, diagnostic, and laboratory testing industries are highly competitive and require an ongoing, extensive search for technological innovation. The industries are characterized by rapidly advancing technologies, intense competition and a strong emphasis on proprietary products. They also require, among other things, the ability to effectively discover, develop, test and obtain regulatory approvals for products, as well as the ability to effectively commercialize, market and promote approved products.
Numerous companies, including major pharmaceutical companies, specialty pharmaceutical companies and specialized biotechnology companies, are engaged in the development, manufacture and marketing of pharmaceutical products competitive with those that we intend to commercialize ourselves and through our partners. Competitors to our diagnostics business include major diagnostic companies, reference laboratories, molecular diagnostic firms, universities and research institutions. Most of these companies have substantially greater financial and other resources, larger research and development staffs and more extensive marketing and manufacturing organizations than ours. This enables them, among other things, to make greater research and development investments and efficiently utilize their research and development costs, as well as their marketing and promotion costs, over a broader revenue base. This also provides our competitors with a competitive advantage in connection with the highly competitive product acquisition and product in-licensing process, which may include auctions in which the highest bidder wins. Our competitors may also have more experience and expertise in obtaining marketing approvals from the FDA and other regulatory authorities. In addition to product development, testing, approval, and promotion, other competitive factors in the pharmaceutical and diagnostics industry include industry consolidation, product quality and price, product technology, reputation, customer service, and access to technical information.
In our clinical laboratory operations, we compete with three types of providers in a highly fragmented and competitive industry: hospital laboratories, physician-office laboratories and other independent clinical laboratories. Our major competitors in the New York metropolitan area are two of the largest national laboratories, Quest Diagnostics and Laboratory Corporation of America. We are much smaller than these national laboratories.
The clinical laboratory business is intensely competitive both in terms of price and service. Pricing of laboratory testing services is often one of the most significant factors used by health care providers and third-party payors in selecting a laboratory. As a result of the clinical laboratory industry undergoing significant consolidation, larger clinical laboratory providers are able to increase cost efficiencies afforded by large-scale automated testing. This consolidation results in greater price competition. We may be unable to increase cost efficiencies sufficiently, if at all, and as a result, our net earnings and cash flows could be negatively impacted by such price competition. Additionally, we may also face changes in fee schedules, competitive bidding for laboratory services or other actions or pressures reducing payment schedules as a result of increased or additional competition.
If our competitors market products that are more effective, safer, easier to use or less expensive than our current products and future product candidates, or that reach the market sooner than our future product candidates, if any, we may not achieve commercial success. In addition, the biopharmaceutical, diagnostic, medical device, and laboratory industries are characterized by rapid technological change. Because our research approach integrates many technologies, it may be difficult for us to stay abreast of the rapid changes in each technology. If we fail to stay at the forefront of technological change, we may be unable to compete effectively. Technological advances or products developed by our competitors may render our technologies or product candidates obsolete or less competitive.
Our product development activities could be delayed or stopped.
We do not know whether our current or planned pre-clinical and clinical studies will be completed on schedule, or at all. Furthermore, we cannot guarantee that our planned pre-clinical and clinical studies will begin on time or at all. The commencement of our planned clinical trials could be substantially delayed or prevented by several factors, including:
▪ |
a limited number of, and competition for, suitable patients with the particular types of disease required for enrollment in our clinical trials or that otherwise meet the protocol’s inclusion criteria and do not meet any of the exclusion criteria; |
▪ |
a limited number of, and competition for, suitable serum or other samples from patients with particular types of disease required for our validation studies; |
▪ |
a limited number of, and competition for, suitable sites to conduct our clinical trials; |
▪ |
delay or failure to obtain FDA or other non-U.S. regulatory authorities’ approval or agreement to commence a clinical trial; |
▪ |
delay or failure to obtain sufficient supplies of the product candidate for our clinical trials; |
27
▪ |
requirements to provide the drugs, diagnostic tests, or medical devices required in our clinical trial protocols or clinical trials at no cost or cost, which may require significant expenditures that we are unable or unwilling to make; |
▪ |
delay or failure to reach agreement on acceptable clinical trial agreement terms or clinical trial protocols with prospective sites or investigators; and |
▪ |
delay or failure to obtain institutional review board (“IRB”) approval to conduct or renew a clinical trial at a prospective site. |
The completion of our clinical trials could also be substantially delayed or prevented by several factors, including:
▪ |
slower than expected rates of patient recruitment and enrollment; |
▪ |
failure of patients to complete the clinical trial; |
▪ |
unforeseen safety issues; |
▪ |
lack of efficacy evidenced during clinical trials; |
▪ |
termination of our clinical trials by one or more clinical trial sites; |
▪ |
inability or unwillingness of patients or medical investigators to follow our clinical trial protocols; and |
▪ |
inability to monitor patients adequately during or after treatment. |
Our clinical trials may be suspended or terminated at any time by the FDA, other regulatory authorities, the IRB for any given site, or us. Additionally, changes in regulatory requirements and guidance may occur and we may need to amend clinical trial protocols to reflect these changes with appropriate regulatory authorities. Amendments may require us to resubmit our clinical trial protocols to IRBs for re-examination, which may impact the costs, timing, or successful completion of a clinical trial. Any failure or significant delay in commencing or completing clinical trials for our product candidates could materially harm our results of operations and financial condition, as well as the commercial prospects for our product candidates.
We currently have limited marketing staff and no pharmaceutical sales or distribution capabilities in the U.S. If we are unable to develop our sales, marketing and distribution capability on our own or through collaborations with marketing partners, we will not be successful in commercializing our pharmaceutical product candidates in the U.S.
We currently have no pharmaceutical marketing, sales or distribution capabilities in the U.S. We intend to establish our sales and marketing organization with technical expertise and supporting distribution capabilities to commercialize our pharmaceutical product candidates, which will be expensive and time-consuming. Any failure or delay in the development of any of our internal sales, marketing, and distribution capabilities would adversely impact the commercialization of our pharmaceutical products. With respect to our existing and future product candidates, we may choose to collaborate with third parties that have direct sales forces and established distribution systems, either to augment our own sales force and distribution systems or in lieu of our own sales force and distribution systems. To the extent that we enter into co-promotion or other licensing arrangements, our product revenue and profit is likely to be lower than if we directly marketed or sold our products. In addition, any revenue we receive will depend in whole or in part upon the efforts of such third parties, which may not be successful and are generally not within our control. If we are unable to enter into such arrangements on acceptable terms or at all, we may not be able to successfully commercialize our existing and future product candidates. If we are not successful in commercializing our existing and future pharmaceutical product candidates, either on our own or through collaborations with one or more third parties, our future product revenue will suffer and we may incur significant additional losses.
Our product candidates may have undesirable side effects and cause our approved products to be taken off the market.
If a product candidate receives marketing approval and we or others later identify undesirable side effects caused by such products:
• |
regulatory authorities may require the addition of labeling statements, specific warnings, a contraindication, or field alerts to physicians and pharmacies; |
• |
regulatory authorities may withdraw their approval of the product and require us to take our approved product off the market; |
• |
we may be required to change the way the product is administered, conduct additional clinical trials, or change the labeling of the product; |
• |
we may have limitations on how we promote our products; |
28
• |
sales of products may decrease significantly; |
• |
we may be subject to litigation or product liability claims; and |
• |
our reputation may suffer. |
Any of these events could prevent us from achieving or maintaining market acceptance of the affected product or could substantially increase our commercialization costs and expenses, which in turn could delay or prevent us from generating significant revenues from its sale.
Our inability to meet regulatory quality standards applicable to our manufacturing and quality processes and to address quality control issues in a timely manner could delay the production and sale of our products or result in recalls of products.
Manufacturing or design defects, unanticipated use of our products, or inadequate disclosure of risks relating to the use of our products could lead to injury or other adverse events. These events could lead to recalls or safety alerts relating to our products (either voluntary or required by governmental authorities) and could result, in certain cases, in the removal of a product from the market. Any recall could result in significant costs as well as negative publicity that could reduce demand for our products. Personal injuries relating to the use of our products can also result in product liability claims being brought against us. In some circumstances, such adverse events could also cause delays in new product approvals.
We are committed to providing high quality products to our customers, and we plan to meet this commitment by working diligently to continue implementing updated and improved quality systems and concepts throughout our organization. We cannot assure you that we will not have quality control issues in the future, which may result in warning letters and citations from the FDA. If we receive any warning letters from the FDA in the future, there can be no assurances regarding the length of time or cost it will take us to resolve such quality issues to our satisfaction and to the satisfaction of the FDA. If our remedial actions are not satisfactory to the FDA, we may have to devote additional financial and human resources to our efforts, and the FDA may take further regulatory actions against us including, but not limited to, assessing civil monetary penalties or imposing a consent decree on us, which could result in further regulatory constraints, including the governance of our quality system by a third party. Our inability to resolve these issues or the taking of further regulatory action by the FDA may weaken our competitive position and have a material adverse effect on our business, results of operations and financial condition.
We manufacture pharmaceutical products in Ireland, Mexico, Spain, and Israel. We also prepare necessary test reagents and assemble and package the cassettes for our point-of-care diagnostic system at our facility in Woburn, Massachusetts. Any quality control issues at our facilities may weaken our competitive position and have a material adverse effect on our business results of operations and financial condition.
As a medical device manufacturer, we are required to register with the FDA and are subject to periodic inspection by the FDA for compliance with its Quality System Regulation (“QSR”) requirements, which require manufacturers of medical devices to adhere to certain regulations, including testing, quality control and documentation procedures. Compliance with applicable regulatory requirements is subject to continual review and is monitored rigorously through periodic inspections by the FDA. In addition, most international jurisdictions have adopted regulatory approval and periodic renewal requirements for medical devices, and we must comply with these requirements in order to market our products in these jurisdictions. In the European Community, we are required to maintain certain ISO certifications in order to sell our products and must undergo periodic inspections by notified bodies to obtain and maintain these certifications. Further, some emerging markets rely on the FDA’s Certificate for Foreign Government (“CFG”) in lieu of their own regulatory approval requirements. Our failure, or our manufacturers’ failure to meet QSR ISO, or any other regulatory requirements or industry standards could delay production of our products and lead to fines, difficulties in obtaining regulatory clearances, recalls or other consequences, which could, in turn, have a material adverse effect on our business, results of operations, and our financial condition.
Failure to establish, and perform to, appropriate quality standards to assure that the highest level of quality is observed in the performance of our testing services could adversely affect the results of our operations and adversely impact our reputation.
The provision of clinical testing services, including anatomic pathology services, and related services, and the design, manufacture and marketing of diagnostic products involve certain inherent risks. The services that we provide and the products that we design, manufacture and market are intended to provide information for healthcare providers in providing patient care. Therefore, users of our services and products may have a greater sensitivity to errors than the users of services or products that are intended for other purposes.
Similarly, negligence in performing our services can lead to injury or other adverse events. We may be sued under physician liability or other liability law for acts or omissions by our pathologists, laboratory personnel and hospital employees
29
who are under the supervision of our hospital-based pathologists. We are subject to the attendant risk of substantial damages awards and risk to our reputation.
Even if we receive regulatory approval or clearance to market our product candidates, the market may not be receptive to our products.
Even if our product candidates obtain marketing approval or clearance, our products may not gain market acceptance among physicians, patients, health care payors and/or the medical community. We believe that the degree of market acceptance will depend on a number of factors, including:
• |
timing of market introduction of competitive products; |
• |
safety and efficacy of our product compared to other products; |
• |
prevalence and severity of any side effects; |
• |
potential advantages or disadvantages over alternative treatments; |
• |
strength of marketing and distribution support; |
• |
price of our products, both in absolute terms and relative to alternative treatments; |
• |
availability of coverage and reimbursement from government and other third-party payors; |
• |
potential product liability claims; |
• |
limitations or warnings contained in a product’s regulatory authority-approved labeling; and |
• |
changes in the standard of care for the targeted indications for any of our product candidates, which could reduce the marketing impact of any claims that we could make following applicable regulatory authority approval. |
In addition, our efforts to educate the medical community and health care payors on the benefits of our product candidates may require significant resources and may never be successful. If our products do not gain market acceptance, it would have a material adverse effect on our business, results of operations, and financial condition.
If our existing and future product candidates are not covered and eligible for reimbursement from government and third party payors, we may not be able to generate significant revenue or achieve or sustain profitability.
The coverage and reimbursement status of newly approved or cleared drugs, diagnostic and laboratory tests is uncertain, and failure of our pharmaceutical products, diagnostic tests or laboratory to be adequately covered by insurance and eligible for adequate reimbursement could limit our ability to market any future product candidates we may develop and decrease our ability to generate revenue from any of our existing and future product candidates that may be approved or cleared. The commercial success of our existing and future product candidates in both domestic and international markets will depend in part on the availability of coverage and adequate reimbursement from third-party payors, including government payors, such as the Medicare and Medicaid programs, managed care organizations, and other third-party payors. The government and other third-party payors are increasingly attempting to contain health care costs by limiting both insurance coverage and the level of reimbursement for new drugs and diagnostic tests and, as a result, they may not cover or provide adequate payment for our product candidates. These payors may conclude that our product candidates are less safe, less effective, or less cost-effective than existing or later-introduced products. These payors may also conclude that the overall cost of the procedure using one of our devices exceeds the overall cost of the competing procedure using another type of device, and third-party payors may not approve our product candidates for insurance coverage and adequate reimbursement.
The failure to obtain coverage and adequate or any reimbursement for our product candidates, or health care cost containment initiatives that limit or restrict reimbursement for our product candidates, may reduce any future product revenue. Even though a drug (not administered by a physician) may be approved by the FDA, this does not mean that a Prescription Drug Plan (“PDP”), a private insurer operating under Medicare Part D, will list that drug on its formulary or will set a reimbursement level. PDPs are not required to make every FDA-approved drug available on their formularies. If our drug products are not listed on sufficient number of PDP formularies or if the PDPs’ levels of reimbursement are inadequate, our business, results of operations, and financial condition could be materially adversely affected.
Additionally, our failure to comply with applicable Medicare, Medicaid and other governmental payor rules could result in our inability to participate in a governmental payor program, our returning funds already paid to us, civil monetary penalties, criminal penalties and/or limitations on the operational function of our laboratory. If we were unable to receive reimbursement under a governmental payor program, a substantial portion of our revenues would be lost, which would adversely affect our results of operations and financial condition.
30
As we evolve from a company primarily involved in development to a company also involved in commercialization of our pharmaceutical and diagnostic products as well as our laboratory testing services, we may encounter difficulties in managing our growth and expanding our operations successfully.
As we advance our product candidates and expand our business, we will need to expand our development, regulatory and commercial infrastructure. As our operations expand, we expect that we will need to manage additional relationships with various third parties, collaborators and suppliers. Maintaining these relationships and managing our future growth will impose significant added responsibilities on members of our management. We must be able to: manage our development efforts and operations effectively; manage our clinical trials effectively; hire, train and integrate additional management, administrative and sales and marketing personnel; improve our managerial, development, operational and finance systems; implement and manage an effective marketing strategy; and expand our facilities, all of which may impose a strain on our administrative and operational infrastructure.
Furthermore, we may acquire additional businesses, products or product candidates that complement or augment our existing business. Integrating any newly acquired business or product could be expensive and time-consuming. We may not be able to integrate any acquired business or product successfully or operate any acquired business profitably. Our future financial performance will depend, in part, on our ability to manage any future growth effectively and our ability to integrate any acquired businesses. We may not be able to accomplish these tasks, and our failure to accomplish any of them could prevent us from successfully growing our company, which would have a material adverse effect on our business, results of operations and financial condition.
Our success is dependent to a significant degree upon the involvement and efforts of our Chairman and Chief Executive Officer, Phillip Frost, M.D.
Our success is dependent to a significant degree upon the efforts of our Chairman and Chief Executive Officer, Phillip Frost, M.D., who is essential to our business. The departure of our CEO for whatever reason or the inability of our CEO to continue to serve in his present capacity could have a material adverse effect upon our business, financial condition, and results of operations. Our CEO has a highly regarded reputation in the pharmaceutical and medical industry and attracts business opportunities and assists both in negotiations with acquisition targets, investment targets, and potential joint venture partners. Our CEO has also provided financing to the Company, both in terms of a credit agreement and equity investments. If we lost his services, our relationships with acquisition and investment targets, joint ventures, and investors may suffer and could cause a material adverse impact on our operations, financial condition, and the value of our Common Stock.
If we fail to attract and retain key management and scientific personnel, we may be unable to successfully operate our business and develop or commercialize our product candidates.
We will need to expand and effectively manage our managerial, operational, sales, financial, development, and other resources in order to successfully operate our business and pursue our research, development, and commercialization efforts for our product candidates. Our success depends on our continued ability to attract, retain, and motivate highly qualified management and pre-clinical and clinical personnel. The loss of the services or support of any of our senior management, particularly Dr. Phillip Frost, our Chairman of the Board and CEO, could delay or prevent the development and commercialization of our product candidates.
If the FDA or other applicable regulatory authorities approve generic products that compete with any of our products or product candidates, the sale of our products or product candidates may be adversely affected.
Once an NDA is approved, the product covered thereby becomes a “listed drug” which, in turn can be relied upon by potential competitors in support of an approval of an abbreviated new drug application, or ANDA, or 505(b)(2) application. U.S. laws and other applicable policies provide incentives to manufacturers to create modified, non-infringing versions of a drug to facilitate the approval of an ANDA or other application for a generic substitute. These manufacturers might only be required to conduct a relatively inexpensive study to show that their product has the same active ingredient(s), dosage form, strength, route of administration, and conditions of use, or labeling, as our product or product candidate and that the generic product is bioequivalent to ours, meaning it is absorbed in the body at the same rate and to the same extent as our product or product candidate. These generic equivalents, which must meet the same quality standards as branded pharmaceuticals, would be significantly less costly than ours to bring to market and companies that produce generic equivalents are generally able to offer their products at lower prices. Thus, after the introduction of a generic competitor, a significant percentage of sales of any branded product is typically lost to the generic product. Accordingly, competition from generic equivalents to our products or product candidates would materially adversely impact our revenues, profitability and cash flows and substantially limit our ability to obtain a return on the investments that we have made in our product candidates.
31
If we fail to acquire and develop other products or product candidates at all or on commercially reasonable terms, we may be unable to diversify or grow our business.
We intend to continue to rely on acquisitions and in-licensing as a source of our products and product candidates for development and commercialization. The success of this strategy depends upon our ability to identify, select, and acquire pharmaceutical and diagnostic products, drug delivery technologies, and medical device product candidates. Proposing, negotiating, and implementing an economically viable product acquisition or license is a lengthy and complex process. We compete for partnering arrangements and license agreements with pharmaceutical, biotechnology and medical device companies, and academic research institutions. Our competitors may have stronger relationships with third parties with whom we are interested in collaborating and/or may have more established histories of developing and commercializing products.
Most of our competitors also have substantially greater financial and other resources than us. As a result, our competitors may have a competitive advantage in entering into partnering arrangements with such third parties, as such partnering arrangements are often decided in an auction process in which the highest bidder wins. In addition, even if we find promising product candidates, and generate interest in a partnering or strategic arrangement to acquire such product candidates, we may not be able to acquire rights to additional product candidates or approved products on terms that we find acceptable, or at all.
We expect that any product candidate to which we acquire rights will require additional development efforts prior to commercial sale, including extensive clinical testing and approval or clearance by the FDA and other non-U.S. regulatory authorities. All product candidates are subject to the risks of failure inherent in pharmaceutical, diagnostic test or medical device product development, including the possibility that the product candidate will not be shown to be sufficiently safe and effective for approval by regulatory authorities. Even if the product candidates are approved or cleared for marketing, we cannot be sure that they would be capable of economically feasible production or commercial success. If we fail to acquire or develop other product candidates that are capable of economically feasible production and commercial success, our business, results of operations and financial condition and cash flows may be materially adversely affected.
We rely on third parties to manufacture and supply our pharmaceutical and diagnostic product candidates.
If our manufacturing partners are unable to produce our products in the amounts that we require, we may not be able to establish a contract and obtain a sufficient alternative supply from another supplier on a timely basis and in the quantities we require. We expect to continue to depend on third-party contract manufacturers for the foreseeable future.
Our product candidates require precise, high quality manufacturing. Any of our contract manufacturers will be subject to ongoing periodic unannounced inspection by the FDA and other non-U.S. regulatory authorities to ensure strict compliance with QSR regulations for devices or cGMPs for drugs, and other applicable government regulations and corresponding standards relating to matters such as testing, quality control, and documentation procedures. If our contract manufacturers fail to achieve and maintain high manufacturing standards in compliance with QSR or cGMPs, we may experience manufacturing errors resulting in patient injury or death, product recalls or withdrawals, delays or interruptions of production or failures in product testing or delivery, delay or prevention of filing or approval of marketing applications for our products, cost overruns, or other problems that could seriously harm our business.
Any performance failure on the part of our contract manufacturers could delay clinical development or regulatory approval or clearance of our product candidates or commercialization of our future product candidates, depriving us of potential product revenue and resulting in additional losses. In addition, our dependence on a third party for manufacturing may adversely affect our future profit margins. Our ability to replace an existing manufacturer may be difficult because the number of potential manufacturers is limited and the FDA must approve any replacement manufacturer before it can begin manufacturing our product candidates. Such approval would result in additional non-clinical testing and compliance inspections. It may be difficult or impossible for us to identify and engage a replacement manufacturer on acceptable terms in a timely manner, or at all.
Independent clinical investigators and contract research organizations that we engage to conduct our clinical trials may not be diligent, careful or timely.
We depend on independent clinical investigators to conduct our clinical trials. Contract research organizations may also assist us in the collection and analysis of data. These investigators and contract research organizations will not be our employees, and we will not be able to control, other than by contract, the amount of resources, including time, that they devote to products that we develop. If independent investigators fail to devote sufficient resources to the development of product candidates or clinical trials, or if their performance is substandard, it will delay the marketing approval or clearance and commercialization of any products that we develop. Further, the FDA requires that we comply with standards, commonly referred to as good clinical practice, for conducting, recording and reporting clinical trials to assure that data and reported results are credible and accurate and that the rights, integrity, and confidentiality of trial subjects are protected. If our
32
independent clinical investigators and contract research organizations fail to comply with good clinical practice, the results of our clinical trials could be called into question and the clinical development of our product candidates could be delayed.
Failure of clinical investigators or contract research organizations to meet their obligations to us or comply with federal regulations and good clinical practice procedures could adversely affect the clinical development of our product candidates and harm our business, results of operations, and financial condition.
If the validity of an informed consent from a subject was to be challenged, it may negatively impact our product development efforts.
We take steps to ensure that all clinical data and genetic and other biological samples are collected from subjects who provide informed consent for the data and samples and we work to ensure that the subjects from whom our data and samples are collected do not retain any proprietary or commercial rights to the data or samples or any discoveries derived from them. However, because we may collect data and samples from countries that are governed by a number of different regulatory regimes, there are many complex legal questions relating to the adequacy of informed consent that we must continually address. The adequacy of any given subject’s informed consent may be challenged in the future, and any given informed consent may prove unlawful or otherwise inadequate for our purposes. Any findings against us, or our clinical collaborators, could obligate us to stop using some of our clinical samples, which in turn may hinder our product development efforts. Such a result would also likely involve legal challenges that may consume our management and financial resources.
Failure to timely or accurately bill for our services could have a material adverse effect on our business.
Billing for laboratory testing services is extremely complicated and is subject to extensive and non-uniform rules and administrative requirements. Depending on the billing arrangement and applicable law, we bill various payors, such as patients, insurance companies, Medicare, Medicaid, physicians, hospitals and employer groups. Changes in laws and regulations could increase the complexity and cost of our billing process. Additionally, in the U.S., third-party payors generally require billing codes on claims for reimbursement that describe the services provided. For laboratory services, the American Medical Association establishes most of the billing codes using a data code set called Current Procedural Terminology, or CPT, codes. Each third-party payor generally develops payment amounts and coverage policies for their beneficiaries or members that ties to the CPT code established for the laboratory test and, therefore, coverage and reimbursement may differ by payor even if the same billing code is reported for claims filing purposes. For laboratory tests without a specific billing code, payors often review claims on a claim-by-claim basis and there are increased uncertainties as to coverage and eligibility for reimbursement.
We intend to implement a new billing system for our laboratory business in 2016. The adoption of the new billing system, which will replace the existing billing system, poses several challenges relating to, among other things, training of personnel, communication of new rules and procedures, changes in corporate culture, migration of data, and the potential instability of the new system. If the remaining implementation of the billing system is delayed, in whole or in part, we would continue to use our current systems which may not be sufficient to support our planned operations and significant upgrades to the current systems may be warranted or required to meet our business needs pending the new billing system implementation.
Incorrect or incomplete documentation and billing information could result in non-payment for services rendered or having to pay back amounts incorrectly billed and collected. Further, the failure to timely or correctly bill could lead to various penalties, including: (1) exclusion from participation in CMS and other government programs; (2) asset forfeitures; (3) civil and criminal fines and penalties; and (4) the loss of various licenses, certificates and authorizations necessary to operate our business, any of which could have a material adverse effect on our results of operations or cash flows.
Failure in our information technology systems, including by cybersecurity attacks or other data security incidents, could significantly increase testing turn-around time or billing processes and otherwise disrupt our operations.
Our operations depend, in part, on the continued performance of our information technology systems. Our information technology systems are potentially vulnerable to physical or electronic break-ins, computer viruses and similar disruptions. In addition, we are in the process of integrating the information technology systems of our recently acquired subsidiaries, and we may experience system failures or interruptions as a result of this process. Sustained system failures or interruption of our systems in one or more of our laboratory operations could disrupt our ability to process laboratory requisitions, perform testing, provide test results in a timely manner and/or bill the appropriate party. Failure of our information technology systems could adversely affect our business, profitability and financial condition.
Although we have information technology security systems, a successful cybersecurity attack or other data security incident could result in the misappropriation and/or loss of confidential or personal information, create system interruptions, or deploy malicious software that attacks our systems. It is possible that a cybersecurity attack might not be noticed for some
33
period of time. The occurrence of a cybersecurity attack or incident could result in business interruptions from the disruption of our information technology systems, or negative publicity resulting in reputational damage with our customers, shareholders and other stakeholders and/or increased costs to prevent, respond to or mitigate cybersecurity events. In addition, the unauthorized dissemination of sensitive personal information or proprietary or confidential information could expose us or other third-parties to regulatory fines or penalties, litigation and potential liability, or otherwise harm our business.
Healthcare plans have taken steps to control the utilization and reimbursement of healthcare services, including clinical test services.
We also face efforts by non-governmental third-party payors, including healthcare plans, to reduce utilization and reimbursement for clinical testing services.
The healthcare industry has experienced a trend of consolidation among healthcare insurance plans, resulting in fewer but larger insurance plans with significant bargaining power to negotiate fee arrangements with healthcare providers, including clinical testing providers. These healthcare plans, and independent physician associations, may demand that clinical testing providers accept discounted fee structures or assume all or a portion of the financial risk associated with providing testing services to their members through capped payment arrangements. In addition, some healthcare plans have been willing to limit the PPO or POS laboratory network to only a single national laboratory to obtain improved fee-for-service pricing. There are also an increasing number of patients enrolling in consumer driven products and high deductible plans that involve greater patient cost-sharing.
The increased consolidation among healthcare plans also has increased the potential adverse impact of ceasing to be a contracted provider with any such insurer. The Health Care Reform Law includes provisions, such as the creation of healthcare exchanges, which may encourage healthcare insurance plans to increase exclusive contracting.
We expect continuing efforts to reduce reimbursements, to impose more stringent cost controls and to reduce utilization of clinical test services. These efforts, including future changes in third-party payor rules, practices and policies, or ceasing to be a contracted provider to a healthcare plan, may have a material adverse effect on our business.
The success of our business may be dependent on the actions of our collaborative partners.
We have entered into and expect in the future to enter into collaborative arrangements with established multi-national pharmaceutical, diagnostic, and medical device companies, which will finance or otherwise assist in the development, manufacture and marketing of products incorporating our technology. We anticipate deriving some revenues from research and development fees, license fees, milestone payments, and royalties from collaborative partners. Our prospects, therefore, may depend to some extent upon our ability to attract and retain collaborative partners and to develop technologies and products that meet the requirements of prospective collaborative partners. In addition, our collaborative partners may have the right to abandon research projects, guide strategy regarding prosecution of relevant patent applications and terminate applicable agreements, including funding obligations, prior to or upon the expiration of the agreed-upon research terms. There can be no assurance that we will be successful in establishing collaborative arrangements on acceptable terms or at all, that collaborative partners will not terminate funding before completion of projects, that our collaborative arrangements will result in successful product commercialization, or that we will derive any revenues from such arrangements. To the extent that we are unable to develop and maintain collaborative arrangements, we would need substantial additional capital to undertake research, development, and commercialization activities on our own.
If we are unable to obtain and enforce patent protection for our products, our business could be materially harmed.
Our success depends, in part, on our ability to protect proprietary methods and technologies that we develop or license under the patent and other intellectual property laws of the U.S. and other countries, so that we can prevent others from unlawfully using our inventions and proprietary information. However, we may not hold proprietary rights to some patents required for us to commercialize our product candidates. Because certain U.S. patent applications are confidential until patents issue, such as applications filed prior to November 29, 2000, or applications filed after such date for which nonpublication has been requested, third parties may have filed patent applications for technology covered by our pending patent applications without our being aware of those applications, and our patent applications may not have priority over those applications. For this and other reasons, we or our third-party collaborators may be unable to secure desired patent rights, thereby losing desired exclusivity. If licenses are not available to us on acceptable terms, we may not be able to market the affected products or conduct the desired activities, unless we challenge the validity, enforceability, or infringement of the third-party patent or otherwise circumvent the third-party patent.
Our strategy depends on our ability to rapidly identify and seek patent protection for our discoveries. In addition, we will rely on third-party collaborators to file patent applications relating to proprietary technology that we develop jointly during
34
certain collaborations. The process of obtaining patent protection is expensive and time-consuming. If our present or future collaborators fail to file and prosecute all necessary and desirable patent applications at a reasonable cost and in a timely manner, our business will be adversely affected. Despite our efforts and the efforts of our collaborators to protect our proprietary rights, unauthorized parties may be able to obtain and use information that we regard as proprietary.
The issuance of a patent does not guarantee that it is valid or enforceable. Any patents we have obtained, or obtain in the future, may be challenged, invalidated, unenforceable, or circumvented. Moreover, the U.S. Patent and Trademark Office (“USPTO”) may commence interference proceedings involving our patents or patent applications. In addition, court decisions may introduce uncertainty in the enforceability or scope of patents owned by biotechnology, pharmaceutical, and medical device companies. Any challenge to, finding of unenforceability or invalidation or circumvention of, our patents or patent applications would be costly, would require significant time and attention of our management, and could have a material adverse effect on our business, results of operations and financial condition.
Our pending patent applications may not result in issued patents. The patent position of pharmaceutical, biotechnology, diagnostic, and medical device companies, including ours, is generally uncertain and involves complex legal and factual considerations. The standards that the USPTO and its foreign counterparts use to grant patents are not always applied predictably or uniformly and can change. There is also no uniform, worldwide policy regarding the subject matter and scope of claims granted or allowable in pharmaceutical, biotechnology, diagnostic, or medical device patents. Accordingly, we do not know the degree of future protection for our proprietary rights or the breadth of claims that will be allowed in any patents issued to us or to others. The legal systems of certain countries do not favor the aggressive enforcement of patents, and the laws of foreign countries may not protect our rights to the same extent as the laws of the U.S. Therefore, the enforceability or scope of our owned or licensed patents in the U.S. or in foreign countries cannot be predicted with certainty, and, as a result, any patents that we own or license may not provide sufficient protection against competitors. We may not be able to obtain or maintain patent protection for our pending patent applications, those we may file in the future, or those we may license from third parties.
While we believe that our patent rights are enforceable, we cannot assure you that any patents that have issued, that may issue, or that may be licensed to us will be enforceable or valid, or will not expire prior to the commercialization of our product candidates, thus allowing others to more effectively compete with us. Therefore, any patents that we own or license may not adequately protect our product candidates or our future products, which could have a material adverse effect on our business, results of operations, and financial condition.
If we are unable to protect the confidentiality of our proprietary information and know-how, the value of our technology and products could be adversely affected.
In addition to patent protection, we also rely on other proprietary rights, including protection of trade secrets, know-how, and confidential and proprietary information. To maintain the confidentiality of trade secrets and proprietary information, we will seek to enter into confidentiality agreements with our employees, consultants, and collaborators upon the commencement of their relationships with us. These agreements generally require that all confidential information developed by the individual or made known to the individual by us during the course of the individual’s relationship with us be kept confidential and not disclosed to third parties. Our agreements with employees also generally provide that any inventions conceived by the individual in the course of rendering services to us shall be our exclusive property.
However, we may not obtain these agreements in all circumstances, and individuals with whom we have these agreements may not comply with their terms. In the event of unauthorized use or disclosure of our trade secrets or proprietary information, these agreements, even if obtained, may not provide meaningful protection, particularly for our trade secrets or other confidential information. To the extent that our employees, consultants, or contractors use technology or know-how owned by third parties in their work for us, disputes may arise between us and those third parties as to the rights in related inventions.
Adequate remedies may not exist in the event of unauthorized use or disclosure of our confidential information. The disclosure of our trade secrets would impair our competitive position and may materially harm our business, financial condition, and results of operations.
We will rely heavily on licenses from third parties. Failure to comply with the provisions of these licenses could result in the loss of our rights under the license agreements.
Many of the patents and patent applications in our patent portfolio are not owned by us, but are licensed from third parties. Such license agreements give us rights for the commercial exploitation of the patents resulting from the respective patent applications, subject to certain provisions of the license agreements. Failure to comply with these provisions could result in the loss of our rights under these license agreements. Our inability to rely on these patents and patent applications,
35
which are the basis of our technology, would have a material adverse effect on our business, results of operations and financial condition.
We license patent rights to certain of our technology from third-party owners. If such owners do not properly maintain or enforce the patents underlying such licenses, our competitive position and business prospects will be harmed.
We have obtained licenses from, among others, INEOS Healthcare, Washington University, UT Southwestern, the President and Fellows of Harvard College, The Scripps Research Institute, Arctic Partners, and Academia Sinica, among others, that are necessary or useful for our business. In addition, we intend to enter into additional licenses of third-party intellectual property in the future. Although our goal is to obtain exclusivity in our licensing transactions, we cannot guarantee that no third parties will step forward and assert inventorship or ownership in our in-licensed patents. In some cases, we may rely on the assurances of our licensors that all ownership rights have been secured and that all necessary agreements are intact or forthcoming.
Our success will depend in part on our ability or the ability of our licensors to obtain, maintain, and enforce patent protection for our licensed intellectual property and, in particular, those patents to which we have secured exclusive rights in our field. We or our licensors may not successfully prosecute the patent applications which are licensed to us. Even if patents issue in respect of these patent applications, we or our licensors may fail to maintain these patents, may determine not to pursue litigation against other companies that are infringing these patents, or may pursue such litigation less aggressively than we would. Without protection for the intellectual property we have licensed, other companies might be able to offer substantially identical products for sale, which could adversely affect our competitive business position and harm our business, results of operations and financial condition.
Our commercial success depends significantly on our ability to operate without infringing the patents and other proprietary rights of third parties.
Other entities may have or obtain patents or proprietary rights that could limit our ability to develop, manufacture, use, sell, offer for sale or import products, or impair our competitive position. In addition, other entities may have or obtain patents or proprietary rights that cover our current research and preclinical studies. While there are statutory exemptions to patent infringement for those who are using third party patented technology in the process of pursuing FDA regulatory approval, the U.S. case law pertaining to such exemptions changes over time. Lawsuits involving such exemptions are very fact intensive and it is currently unclear under U.S. case law whether preclinical studies would always qualify for such an exemption, and whether such exemptions would apply to research tools. To the extent that our current research and preclinical studies may be covered by the patent rights of others, the risk of suit may continue after such patents expire because the statute of limitations for patent infringement runs for six years. To the extent that a third party develops and patents technology that covers our products, we may be required to obtain licenses to that technology, which licenses may not be available or may not be available on commercially reasonable terms, if at all. If licenses are not available to us on acceptable terms, we will not be able to market the affected products or conduct the desired activities, unless we challenge the validity, enforceability or infringement of the third-party patent, or circumvent the third-party patent, which would be costly and would require significant time and attention of our management. Third parties may have or obtain by license or assignment valid and enforceable patents or proprietary rights that could block us from developing products using our technology. Our failure to obtain a license to any technology that we require may materially harm our business, financial condition, and results of operations.
If we become involved in patent litigation or other proceedings related to a determination of rights, we could incur substantial costs and expenses, substantial liability for damages or be required to stop our product development and commercialization efforts.
Third parties may sue us for infringing their patent rights. Likewise, we may need to resort to litigation to enforce a patent issued or licensed to us or to determine the scope and validity of proprietary rights of others. In addition, a third-party may claim that we have improperly obtained or used its confidential or proprietary information. Furthermore, in connection with our third-party license agreements, we generally have agreed to indemnify the licensor for costs incurred in connection with litigation relating to intellectual property rights. The cost to us of any litigation or other proceeding relating to intellectual property rights, even if resolved in our favor, could be substantial, and the litigation would divert our management’s efforts. Some of our competitors may be able to sustain the costs of complex patent litigation more effectively than we can because they have substantially greater resources. Uncertainties resulting from the initiation and continuation of any litigation could limit our ability to continue our operations. Our involvement in patent litigation and other proceedings could have a material adverse effect on our business, results of operations, and financial condition.
36
If any parties successfully claim that our creation or use of proprietary technologies infringes upon their intellectual property rights, we might be forced to pay damages, potentially including treble damages, if we are found to have willfully infringed on such parties’ patent rights. In addition to any damages we might have to pay, a court could require us to stop the infringing activity or obtain a license. Any license required under any patent may not be made available on commercially acceptable terms, if at all. In addition, such licenses are likely to be non-exclusive and, therefore, our competitors may have access to the same technology licensed to us. If we fail to obtain a required license and are unable to design around a patent, we may be unable to effectively market some of our technology and products, which could limit our ability to generate revenues or achieve profitability and possibly prevent us from generating revenue sufficient to sustain our operations.
We have faced, and may in the future face, intellectual property infringement claims that could be time-consuming and costly to defend, and could result in our loss of significant rights and the assessment of treble damages.
We may from time to time receive notices of claims of infringement and misappropriation or misuse of other parties’ proprietary rights. Some of these additional claims may also lead to litigation. We cannot assure you that we will prevail in such actions, or that other actions alleging misappropriation or misuse by us of third-party trade secrets, infringement by us of third-party patents and trademarks or the validity of our patents, will not be asserted or prosecuted against us.
We may also initiate claims to defend our intellectual property or to seek relief on allegations that we use, sell, or offer to sell technology that incorporates third party intellectual property. Intellectual property litigation, regardless of outcome, is expensive and time-consuming, could divert management’s attention from our business and have a material negative effect on our business, operating results or financial condition. If there is a successful claim of infringement against us, we may be required to pay substantial damages (including treble damages if we were to be found to have willfully infringed a third party’s patent) to the party claiming infringement, develop non-infringing technology, stop selling our tests or using technology that contains the allegedly infringing intellectual property or enter into royalty or license agreements that may not be available on acceptable or commercially practical terms, if at all. Our failure to develop non-infringing technologies or license the proprietary rights on a timely basis could harm our business.
It is possible that a third party or patent office might take the position that one or more patents or patent applications constitute prior art in the field of genomic-based diagnostics. In such a case, we might be required to pay royalties, damages and costs to firms who own the rights to these patents, or we might be restricted from using any of the inventions claimed in those patents.
We may become subject to product liability for our diagnostic tests, clinical trials, pharmaceutical products and medical device products.
Our success depends on the market’s confidence that we can provide reliable, high-quality pharmaceuticals, medical devices, and diagnostics tests. Our reputation and the public image of our products or technologies may be impaired if our products fail to perform as expected or our products are perceived as difficult to use. Our products are complex and may develop or contain undetected defects or errors. Furthermore, if a future product candidate harms people, or is alleged to be harmful, we may be subject to costly and damaging product liability claims brought against us by clinical trial participants, consumers, health care providers, corporate partners or others. We have product liability insurance covering commercial sales of current products and our ongoing clinical trials. Any defects or errors could lead to the filing of product liability claims, which could be costly and time-consuming to defend and result in substantial damages. If we experience a sustained material defect or error, this could result in loss or delay of revenues, delayed market acceptance, damaged reputation, diversion of development resources, legal claims, increased insurance costs or increased service and warranty costs, any of which could materially harm our business. We cannot assure you that our product liability insurance would protect our assets from the financial impact of defending a product liability claim. A product liability claim could have a serious adverse effect on our business, financial condition and results of operations.
Adverse results in material litigation matters or governmental inquiries could have a material adverse effect upon our business and financial condition.
We may from time to time become subject in the ordinary course of business to material legal action related to, among other things, intellectual property disputes, professional liability, contractual and employee-related matters, as well as inquiries from governmental agencies and Medicare or Medicaid carriers requesting comment and information on allegations of billing irregularities and other matters that are brought to their attention through billing audits, third parties or other sources. The health care industry is subject to substantial federal and state government regulation and audit. Legal actions could result in substantial monetary damages as well as damage to the Company’s reputation with customers, which could have a material adverse effect upon our results of operations and financial position.
RISKS RELATED TO REGULATORY COMPLIANCE
37
Our ability to successfully operate our laboratories and develop and commercialize certain of our diagnostic tests and LDTs will depend on our ability to maintain required regulatory licensures and comply with all the CLIA requirements.
In order to successfully operate our laboratory business and offer certain of our diagnostic tests and LDTs, we must maintain our CLIA certification and comply with all the CLIA requirements. CLIA is designed to ensure the quality and reliability of clinical laboratories by mandating specific standards in the areas of personnel qualifications, administration and participation in proficiency testing, patient test management, quality control, quality assurance and inspections. The sanction for failure to comply with CLIA requirements may be suspension, revocation or limitation of a laboratory’s CLIA certificate, which is necessary to conduct business, as well as significant fines and/or criminal penalties. Laboratories must undergo on-site surveys at least every two years, which may be conducted by the Federal CLIA program or by a private CMS approved accrediting agency such as CAP, among others. Our laboratories are also subject to regulation of laboratory operations under state clinical laboratory laws as will be any new CLIA-certified laboratory that we establish or acquire. State clinical laboratory laws may require that laboratories and/or laboratory personnel meet certain qualifications, specify certain quality controls or require maintenance of certain records. Certain states, such as California, Florida, Maryland, New York, Pennsylvania and Rhode Island, require that laboratories obtain licenses to test specimens from patients residing in those states and additional states may require similar licenses in the future. If we are unable to obtain and maintain licenses from states where required, we will not be able to process any samples from patients located in those states. Only Washington and New York States are exempt under CLIA, as these states have established laboratory quality standards at least as stringent as CLIA’s. Potential sanctions for violation of these statutes and regulations include significant fines and the suspension or loss of various licenses, certificates and authorizations, which could adversely affect our business and results of operations.
If we fail to comply with CLIA requirements, HHS or state agencies could require us to cease diagnostic testing. Even if it were possible for us to bring our laboratories back into compliance after failure to comply with such requirements, we could incur significant expenses and potentially lose revenues in doing so. Moreover, new interpretations of current regulations or future changes in regulations under CLIA may make it difficult or impossible for us to comply with the CLIA classification, which would significantly harm our business and materially adversely affect our financial condition.
The regulatory approval process is expensive, time consuming and uncertain and may prevent us or our collaboration partners from obtaining approvals for the commercialization of some or all of our product candidates.
The research, testing, manufacturing, labeling, approval, selling, marketing, and distribution of drug products, diagnostic products, or medical devices are subject to extensive regulation by the FDA and other non-U.S. regulatory authorities, which regulations differ from country to country. In general, we are not permitted to market our product candidates in the U.S. until we receive approval of a NDA, a clearance letter under the premarket notification process, or 510(k) process, or an approval of a PMA from the FDA. We have only submitted one NDA to date, which has not yet been approved. We have not received marketing approval or clearance for any of our diagnostic product candidates, other than a CE Mark for our point-of-care PSA test and a CE Mark for our 4Kscore test. Obtaining approval of a NDA or PMA can be a lengthy, expensive, and uncertain process. With respect to medical devices, while the FDA reviews and clears a premarket notification in as little as three months, there is no guarantee that our products will qualify for this more expeditious regulatory process, which is reserved for Class I and II devices, nor is there any assurance that even if a device is reviewed under the 510(k) process that the FDA will review it expeditiously or determine that the device is substantially equivalent to a lawfully marketed non-PMA device. If the FDA fails to make this finding, then we cannot market the device. In lieu of acting on a premarket notification, the FDA may seek additional information or additional data which would further delay our ability to market the product. Furthermore, we are not permitted to make changes to a device approved through the PMA or 510(k) which affects the safety or efficacy of the device without first submitting a supplement application to the PMA and obtaining FDA approval or cleared premarket notification for that supplement. In some cases, the FDA may require clinical trials to support a supplement application. In addition, failure to comply with FDA, non-U.S. regulatory authorities, or other applicable U.S. and non-U.S. regulatory requirements may, either before or after product approval or clearance, if any, subject our company to administrative or judicially imposed sanctions, including, but not limited to the following:
▪ |
restrictions on the products, manufacturers, or manufacturing process; |
▪ |
adverse inspectional observations (Form 483), warning letters, or non-warning letters incorporating inspectional observations; |
▪ |
civil and criminal penalties; |
▪ |
injunctions; |
▪ |
suspension or withdrawal of regulatory approvals or clearances; |
▪ |
product seizures, detentions, or import bans; |
38
▪ |
voluntary or mandatory product recalls and publicity requirements; |
▪ |
total or partial suspension of production; |
▪ |
imposition of restrictions on operations, including costly new manufacturing requirements; and |
▪ |
refusal to approve or clear pending NDAs or supplements to approved NDAs, applications or pre-market notifications. |
Regulatory approval of an NDA or NDA supplement, PMA, PMA supplement or clearance pursuant to a pre-market notification is not guaranteed, and the approval or clearance process, as the case may be, is expensive and may, especially in the case of an NDA or PMA application, take several years. The FDA also has substantial discretion in the drug and medical device approval and clearance process. Despite the time and expense exerted, failure can occur at any stage, and we could encounter problems that cause us to abandon clinical trials or to repeat or perform additional pre-clinical studies and clinical trials. The number of pre-clinical studies and clinical trials that will be required for FDA approval or clearance varies depending on the drug or medical device candidate, the disease or condition that the drug or medical device candidate is designed to address, and the regulations applicable to any particular drug or medical device candidate. The FDA can delay, limit or deny approval or clearance of a drug or medical device candidate for many reasons, including:
▪ |
a drug candidate may not be deemed safe or effective; |
▪ |
a medical device candidate may not be deemed to be substantially equivalent to a lawfully marketed non-PMA device, in the case of a premarket notification; |
▪ |
the FDA may not find the data from pre-clinical studies and clinical trials sufficient; |
▪ |
the FDA may not approve our or our third-party manufacturer’s processes or facilities; or |
▪ |
the FDA may change its approval or clearance policies or adopt new regulations. |
Beyond these risks, there is also a possibility that our licensees or collaborators could decide to discontinue a study at any time for commercial, scientific or other reasons.
Regulation by governmental authorities in the U.S. and other countries may be a significant factor in how we develop, test, produce and market our diagnostic test products. Diagnostic tests like ours may not fall squarely within the regulatory approval process for pharmaceutical or device products as described above, and the regulatory pathway is not as clear. It is possible that the diagnostic products developed by us or our collaborators will be regulated as medical devices by the FDA and comparable agencies of other countries and require either PMA or 510(k) clearance from the FDA prior to marketing. Some companies that have successfully commercialized diagnostic tests for various conditions and disease states have not sought clearance or approval for such tests through the traditional 510(k) or PMA processes, and have instead utilized a process involving LDTs through a CLIA- certified laboratory. CLIA is a federal law that regulates clinical laboratories that perform testing on specimens derived from humans for the purpose of providing information for diagnostic, preventative or treatment purpose. In such instances, the CLIA lab is solely responsible for the development, validation and commercialization of the assay.
Such LDT testing is currently under the purview of CMS and state agencies that provide oversight of the safe and effective use of LDTs. However, the FDA has consistently asserted that it has the regulatory authority to regulate LDTs despite historically exercising enforcement discretion. In furtherance of that position, the FDA issued two draft guidance documents in October 2014: Framework for Regulatory Oversight of Laboratory Developed Tests (the “Framework Guidance”); and (2) FDA Notification and Medical Device Reporting for Laboratory Developed Tests (the “Notification Guidance”). The Framework Guidance outlines the FDA’s plan to adopt over time a risk-based approach to regulating LDTs whereby different classifications of LDTs would be subject to different levels of FDA oversight and enforcement, including, for example, prohibitions on adulteration and misbranding, establishment registration and device listing, premarket notification, banned devices, records and reports, good manufacturing practices, adverse event reporting, premarket review of safety, effectiveness, and clinical validity, and quality system requirements. The Notification Guidance is intended to explain how clinical laboratories should notify the FDA of the LDTs they develop and how to satisfy Medical Device Reporting requirements. If finalized, the Framework Guidance and the Notification Guidance may have a materially adverse effect on the time, cost, and risk associated with the Company’s development and commercialization of LDTs for the U.S. market, and there can be no assurance that clearances or approvals sought by the Company will be granted and maintained. However, the FDA’s authority to regulate LDTs continues to be challenged, and the timeline and process for finalizing the draft guidance documents is unknown. We will continue to monitor changes to all domestic and international LDT regulatory policy so as to ensure compliance with the current regulatory scheme.
39
Even if we obtain marketing approvals or clearances for our product candidates, the terms of approvals and ongoing regulation of our products may limit how we manufacture and market our product candidates, which could materially impair our ability to generate anticipated revenues.
Once regulatory approval has been granted to market a product, the approved or cleared product and its manufacturer are subject to continual review. Any approved or cleared product may only be promoted for its indicated uses. In addition, if the FDA or other non-U.S. regulatory authorities approve any of our product candidates for marketing, the labeling, packaging, adverse event reporting, storage, advertising, and promotion for the product will be subject to extensive regulatory requirements. We and the manufacturers of our products are also required to comply with current Good Manufacturing Practices (“cGMP”) regulations or the FDA’s QSR regulations, which include requirements relating to quality control and quality assurance as well as the corresponding maintenance of records and documentation. Moreover, device manufacturers are required to report adverse events by filing Medical Device Reports with the FDA, which reports are publicly available.
Further, regulatory agencies must approve manufacturing facilities before they can be used to manufacture our products, and these facilities are subject to ongoing regulatory inspection. If we fail to comply with the regulatory requirements of the FDA and other non-U.S. regulatory authorities, or if previously unknown problems with our products, manufacturers, or manufacturing processes are discovered, we could be subject to administrative or judicially imposed sanctions. Furthermore, any limitation on indicated uses for a product candidate or our ability to manufacture and promote a product candidate could significantly and adversely affect our business, results of operations, and financial condition.
In addition, the FDA and other non-U.S. regulatory authorities may change their policies and additional regulations may be enacted that could prevent or delay marketing approval or clearance of our product candidates. We cannot predict the likelihood, nature or extent of government regulation that may arise from future legislation or administrative action, either in the U.S. or abroad. If we are not able to maintain regulatory compliance, we would likely not be permitted to market our future product candidates and we may not achieve or sustain profitability, which would materially impair our ability to generate anticipated revenues.
If we fail to comply with complex and rapidly evolving laws and regulations, we could suffer penalties, be required to pay substantial damages or make significant changes to our operations.
We are subject to numerous federal and state regulations, including, but not limited to:
• |
federal and state laws applicable to billing and claims payment; |
• |
federal and state laboratory anti-mark-up laws; |
• |
federal and state anti-kickback laws; |
• |
physician self-referral law; |
• |
federal and state false claims laws; |
• |
federal self-referral and financial inducement prohibition laws, commonly known as the Stark Law, and the state equivalents; |
• |
federal and state laws governing laboratory licensing and testing, including CLIA; |
• |
federal and state laws governing the development, use and distribution of LDTs; |
• |
HIPAA, along with the revisions to HIPPA as a result of the HITECH Act, and analogous state laws; |
• |
federal, state and foreign regulation of privacy, security, electronic transactions and identity theft; |
• |
federal, state and local laws governing the handling, transportation and disposal of medical and hazardous waste; |
• |
Occupational Safety and Health Administration rules and regulations; |
• |
changes to laws, regulations and rules as a result of the Health Care Reform Law; and |
• |
changes to other federal, state and local laws, regulations and rules, including tax laws. |
If we fail to comply with existing or future applicable laws and regulations, we could suffer civil or criminal penalties, including the loss of our licenses to operate our laboratories and our ability to participate in federal and state healthcare programs. Although we believe that we are substantially compliant with all existing statutes and regulations applicable to our business, different interpretations and enforcement policies of these laws and regulations could subject our current practices to allegations of impropriety or illegality, or could require us to make significant changes to our operations. In addition, we
40
cannot predict the impact of future legislation and regulatory changes on our business or assure that we will be able to obtain or maintain the regulatory approvals required to operate our business.
As a result of political, economic, and regulatory influences, the healthcare delivery industry in the U.S. is under intense scrutiny and subject to fundamental changes. We cannot predict which reform proposals will be adopted, when they may be adopted, or what impact they may have on us. The costs associated with complying with federal and state regulations could be significant and the failure to comply with any such legal requirements could have a material adverse effect on our financial condition, results of operations, and liquidity.
Failure to maintain the security of patient-related information or compliance with security requirements could damage our reputation with customers, cause us to incur substantial additional costs and become subject to litigation.
Pursuant to HIPAA, and certain similar state laws, we must comply with comprehensive privacy and security standards with respect to the use and disclosure of protected health information. Under the HITECH amendments to HIPAA, HIPAA was expanded to require certain data breach notification, to extend certain HIPAA privacy and security standards directly to business associates, to heighten penalties for noncompliance, and enhance enforcement efforts.
In March 2014 CareEvolve, Bio-Reference’s wholly-owned connectivity subsidiary, became aware that there had been a HIPAA breach with regard to one of its servers managed at an internet service provider site called XAND. CareEvolve immediately identified and resolved the breach issue, but in the meantime an Internet data googlebot, a data collection “robot” operated by Google, Inc. had briefly acquired data from a server and made it available to Internet searches. To the best of our knowledge, there were no known disclosures of this Patient Health Information (“PHI”) to unauthorized parties and Bio-Reference took immediate steps to have the PHI removed from the Internet. Bio-Reference self-reported this incident to the appropriate government agency, the Office of Civil Rights (“OCR”) and is awaiting further discussions, investigation and action by OCR.
We receive certain personal and financial information about our clients and their patients. In addition, we depend upon the secure transmission of confidential information over public networks. While we take all reasonable and prudent steps to protect this protected information, a compromise in our security systems that results in client or patient personal information being obtained by unauthorized persons or our failure to comply with security requirements for financial transactions could adversely affect our reputation with our clients and result in litigation against us or the imposition of penalties, all of which may adversely impact our results of operations, financial condition and liquidity.
Failure to comply with environmental, health and safety laws and regulations, including the Federal Occupational Safety and Health Administration Act, the Needlestick Safety and Prevention Act and the Comprehensive Medical Waste Management Act, could result in fines and penalties and loss of licensure, and have a material adverse effect upon our business.
We are subject to licensing and regulation under federal, state and local laws and regulations relating to the protection of the environment and human health and safety, including laws and regulations relating to the handling, transportation and disposal of medical specimens, infectious and hazardous waste and radioactive materials, as well as regulations relating to the safety and health of laboratory employees. The Federal Occupational Safety and Health Administration has established extensive requirements relating to workplace safety for health care employers, including clinical laboratories, whose workers may be exposed to blood-borne pathogens such as HIV and the hepatitis B virus. These requirements, among other things, require work practice controls, protective clothing and equipment, training, medical follow-up, vaccinations and other measures designed to minimize exposure to, and transmission of, blood-borne pathogens. In addition, the Needlestick Safety and Prevention Act requires, among other things, that we include in our safety programs the evaluation and use of engineering controls such as safety needles if found to be effective at reducing the risk of needlestick injuries in the workplace.
Waste management is subject to federal and state regulations governing the transportation and disposal of medical waste including bodily fluids. Federal regulations require licensure of interstate transporters of medical waste. In New Jersey, we are subject to the Comprehensive Medical Waste Management Act (“CMWMA”), which requires us to register as a generator of special medical waste. All of our medical waste is disposed of by a licensed interstate hauler. The hauler provides a manifest of the disposition of the waste products as well as a certificate of incineration, which is retained by us. These records are audited by the State of New Jersey on a yearly basis. We are also subject to the Federal Hazardous materials transportation law, 49 U.S.C. 5101 et seq., and the Hazardous Materials Regulations (“HMR”), 49 CFR parts 171-180. The federal government has classified hazardous medical waste as hazardous materials for the purpose of regulation. These regulations preempt state regulation, which must be “substantively the same,” “the non-federal requirement must conform “in every significant respect to the federal requirement. Editorial and other similar de minimis changes are permitted,” 49 CFR 107.202(d).
41
Failure to comply with such federal, state and local laws and regulations could subject us to denial of the right to conduct business, fines, criminal penalties and/or other enforcement actions, any of which could have a material adverse effect on our business. In addition, compliance with future legislation could impose additional requirements us, which may be costly.
Our failure or the failure of third-party payors or physicians to comply with ICD-10-CM Code Set, and our failure to comply with other emerging electronic transaction standards could adversely impact our business.
We are within the assessment and inventory phase to adopt the ICD-10-CM Code Set issued by HHS on January 16, 2009. Compliance with the ICD-10-CM Code Set was required to be in place by October 1, 2015. The Company will continue its assessment of information systems, applications and processes for compliance with these requirements. Clinical laboratories are typically required to submit health care claims with diagnosis codes to third party payors. The diagnosis codes must be obtained from the ordering physician. Our failure or the failure of third party payors or physicians to transition within the required timeframe could have an adverse impact on reimbursement, days sales outstanding and cash collections.
Also, the failure of our IT systems to keep pace with technological advances may significantly reduce our revenues or increase our expenses. Public and private initiatives to create healthcare information technology (“HCIT”) standards and to mandate standardized clinical coding systems for the electronic exchange of clinical information, including test orders and test results, could require costly modifications to our existing HCIT systems. While we do not expect HCIT standards to be adopted or implemented without adequate time to comply, if we fail to adopt or delay in implementing HCIT standards, we could lose customers and business opportunities.
Failure to comply with complex federal and state laws and regulations related to submission of claims for clinical laboratory services could result in significant monetary damages and penalties and exclusion from the Medicare and Medicaid programs.
We are subject to extensive federal and state laws and regulations relating to the submission of claims for payment for clinical laboratory services, including those that relate to coverage of our services under Medicare, Medicaid and other governmental health care programs, the amounts that may be billed for our services and to whom claims for services may be submitted. These rules may also affect the Company in light of the practice management products that we market, to the extent that these products are considered to affect the manner in which our customers’ submit their own claims for services. Submission of our claims is particularly complex because we provide both anatomic pathology services and clinical laboratory tests, which generally are paid using different reimbursement principles. The clinical laboratory tests are often paid under a clinical laboratory fee schedule, and the anatomic pathology services are often paid under a physician fee schedule.
Our failure to comply with applicable laws and regulations could result in our inability to receive payment for our services or result in attempts by third-party payors, such as Medicare and Medicaid, to recover payments from us that have already been made. Submission of claims in violation of certain statutory or regulatory requirements can result in penalties, including substantial civil money penalties for each item or service billed to Medicare in violation of the legal requirement, and exclusion from participation in Medicare and Medicaid. Government authorities may also assert that violations of laws and regulations related to submission or causing the submission of claims violate the federal False Claims Act (“FCA”) or other laws related to fraud and abuse, including submission of claims for services that were not medically necessary. Violations of the FCA could result in enormous economic liability. The FCA provides that all damages are trebled, and each false claim submitted is subject to a penalty of up to $11,000. For example, we could be subject to FCA liability if it was determined that the services we provided were not medically necessary and not reimbursable, particularly if it were asserted that we contributed to the physician’s referrals of unnecessary services to us. It is also possible that the government could attempt to hold us liable under fraud and abuse laws for improper claims submitted by an entity for services that we performed if we were found to have knowingly participated in the arrangement that resulted in submission of the improper claims.
Changes in regulation and policies, including increasing downward pressure on health care reimbursement, may adversely affect reimbursement for diagnostic services and could have a material adverse impact on our business.
Reimbursement levels for health care services are subject to continuous and often unexpected changes in policies, and we face a variety of efforts by government payors to reduce utilization and reimbursement for diagnostic testing services. Changes in governmental reimbursement may result from statutory and regulatory changes, retroactive rate adjustments, administrative rulings, competitive bidding initiatives, and other policy changes.
The U.S. Congress has considered, at least yearly in conjunction with budgetary legislation, changes to one or both of the Medicare fee schedules under which we receive reimbursement, which include the physician fee schedule for anatomical pathology services, and the clinical laboratory fee schedule for our clinical laboratory services. For example, currently there is no copayment or coinsurance required for clinical laboratory services, although there is for our physician services. However, Congress has periodically considered imposing a 20 percent coinsurance on laboratory services. If enacted, this would require
42
us to attempt to collect this amount from patients, although in many cases the costs of collection would exceed the amount actually received.
Our reimbursement for our pathology services is paid primarily under the physician fee schedule of Medicare and Medicaid and is therefore governed by a complex formula, referred to as the Sustainable Growth Rate, or SGR. As the use of this formula could result in a significant reduction in reimbursement for all physician services, Congress usually acts each year to prevent the full amount of such reductions from taking effect. In 2011, Congress acted to prevent reductions in for 2012, and on January 1, 2013, Congress acted to prevent significant reductions for 2013. The SGR has currently been postponed until March 2014 and Congress continues to work on both a short term and a long term fix to this annual problem. If Congress fails to take such action in the future, implementation of this formula could adversely affect our business.
The Center for Medicare and Medicaid Services (“CMS”) pays laboratories on the basis of a fee schedule that is reviewed and re-calculated on an annual basis. CMS may change the fee schedule upward or downward on billing codes that we submit for reimbursement on a regular basis. Our revenue and business may be adversely affected if the reimbursement rates associated with such codes are reduced. Even when reimbursement rates are not reduced, policy changes add to our costs by increasing the complexity and volume of administrative requirements. Medicaid reimbursement, which varies by state, is also subject to administrative and billing requirements and budget pressures. Recently, state budget pressures have caused states to consider several policy changes that may impact our financial condition and results of operations, such as delaying payments, reducing reimbursement, restricting coverage eligibility and service coverage, and imposing taxes on our services.
Change in the billing and/or reimbursement procedures by the federal government could affect our ability to be paid as we have in the past for services rendered.
CMS has changed or discussed making changes to certain types of reimbursement which could affect our rate of reimbursement. Certain cases are comprised of both a technical component (“TC”) and a professional component (“PC”). In certain specified areas of testing, primarily in the area of anatomic pathology, CMS has determined that some providers have over-utilized these testing procedures and CMS has introduced changes in reimbursement policies to discourage over-utilization. While we do not currently over-utilize services for self-gain, we are always subject to review by CMS and cannot be certain that CMS won’t interpret our practices differently than we do.
CMS has announced planned changes in the area of Molecular Diagnostics’ reimbursement, primarily designed to improve transparency in billing. Molecular Diagnostics is a rapidly changing and evolving area of clinical testing. Whereas other areas of clinical testing are well vetted and established with specific codes for reimbursement, Molecular Diagnostics has moved at a faster pace than CMS can proceed. Clinical laboratories accordingly use a process called cross-walking to get reimbursed by CMS. Cross-walking requires that the clinical laboratory identify the individual processes used to process the patient’s specimen and identify diagnostic results that are already reimbursed in established tests. CMS seeks to specifically identify the testing routine being done and reimburse providers universally for the test actually being performed. CMS has not established all of the molecular diagnostic tests that will be included in this revised schedule for reimbursement and it has not determined how much will be reimbursed to providers for these tests. We expect CMS to implement fair and reasonable reimbursement for such tests, but until such pricing decisions are disclosed we cannot be certain what CMS will finally implement.
Effective July 1, 2012, CMS eliminated an exemption that had been in place since 1999, which allowed commercial laboratories to bill for certain diagnostic tests performed on in-patient and certain outreach recipients by commercial laboratories. From 1999 through July 1, 2012, commercial laboratories were allowed to bill CMS for such tests despite the fact that the recipient was a hospital patient as long as the hospital had been submitting such tests for diagnosis to commercial laboratories prior to 1999. Upon termination of the exemption, we were required to find out from the hospital submitting the test whether the recipient’s bill for diagnostic testing will be reimbursed by the hospital or should be billed to CMS. We have systems in place to manage this change, but these systems are dependent upon our getting proper information from the hospital clients.
The federal government is faced with significant economic decisions in the coming years. Some solutions being offered in the government could substantially change the way laboratory testing is reimbursed by government entities. We cannot be certain what or how any such government changes may affect our business.
Medicare legislation and future legislative or regulatory reform of the health care system may affect our ability to sell our products profitably.
In the U.S., there have been a number of legislative and regulatory initiatives, at both the federal and state government levels, to change the healthcare system in ways that, if approved, could affect our ability to sell our products and provide our laboratory services profitably. While many of the proposed policy changes require congressional approval to implement, we
43
cannot assure you that reimbursement payments under governmental and private third party payor programs will remain at levels comparable to present levels or will be sufficient to cover the costs allocable to patients eligible for reimbursement under these programs. Any changes that lower reimbursement rates under Medicare, Medicaid or private payor programs could negatively affect our business.
Most significantly, on March 23, 2010, President Obama signed into law both the Patient Protection and Affordable Care Act (the “Affordable Care Act”) and the reconciliation law known as Health Care and Education Affordability Reconciliation Act (the “Reconciliation Act”) and, combined we refer to both Acts as the “2010 Health Care Reform Legislation.” The constitutionality of the 2010 Health Care Reform Legislation was confirmed on June 28, 2012 by the Supreme Court of the United States (the “Supreme Court”). Specifically, the Supreme Court upheld the individual mandate and includes changes to extend medical benefits to those who currently lack insurance coverage. Extending coverage to a large population could substantially change the structure of the health insurance system and the methodology for reimbursing medical services, drugs and devices. These structural changes could entail modifications to the existing system of third-party payors and government programs, such as Medicare and Medicaid, the creation of a government-sponsored healthcare insurance source, or some combination of both, as well as other changes. Additionally, restructuring the coverage of medical care in the U.S. could impact the reimbursement for diagnostic tests. If reimbursement for our diagnostic tests is substantially less than we or our clinical laboratory customers expect, or rebate obligations associated with them are substantially increased, our business could be materially and adversely impacted.
Beyond coverage and reimbursement changes, the 2010 Health Care Reform Legislation subjects manufacturers of medical devices to an excise tax of 2.3% on certain U.S. sales of medical devices in January 2013. This excise tax will likely increase our expenses in the future.
Further, the 2010 Health Care Reform Legislation includes the Physician Payments Sunshine Act, which, in conjunction with its implementing regulations, requires manufacturers of certain drugs, biologics, and devices that are covered by Medicare and Medicaid to record all transfers of value to physicians and teaching hospitals starting on August 1, 2013 and to begin reporting the same for public disclosure to the Centers for Medicare and Medicaid Services by March 31, 2014. Several other states and a number of countries worldwide have adopted or are considering the adoption of similar transparency laws. The failure to report appropriate data may result in civil or criminal fines and/or penalties.
Additionally, the 2010 Health Care Reform Legislation includes significant new fraud and abuse measures, including required disclosures under Physician Payments Sunshine Act described above, lower thresholds for violations and increasing potential penalties for such violations. Federal funding available for combating health care fraud and abuse generally has increased. While we seek to conduct our business in compliance with all applicable laws and regulations, many of the laws and regulations applicable to our business, particularly those relating to billing and reimbursement of tests and those relating to relationships with physicians, hospitals and patients, contain language that has not been interpreted by courts. We must rely on our interpretation of these laws and regulations based on the advice of our counsel and regulatory or law enforcement authorities may not agree with our interpretation of these laws and regulations and may seek to enforce legal remedies or penalties against us for violations. From time to time we may need to change our operations, particularly pricing or billing practices, in response to changing interpretations of these laws and regulations or regulatory or judicial determinations with respect to these laws and regulations. These occurrences, regardless of their outcome, could damage our reputation and harm important business relationships that we have with healthcare providers, payors and others. Furthermore, if a regulatory or judicial authority finds that we have not complied with applicable laws and regulations, we could be required to refund amounts that were billed and collected in violation of such laws and regulations. In addition, we may voluntarily refund amounts that were alleged to have been billed and collected in violation of applicable laws and regulations. In either case, we could suffer civil and criminal damages, fines and penalties, exclusion from participation in governmental healthcare programs and the loss of licenses, certificates and authorizations necessary to operate our business, as well as incur liabilities from third-party claims, all of which could harm our operating results and financial condition. Moreover, regardless of the outcome, if we or physicians or other third parties with whom we do business are investigated by a regulatory or law enforcement authority we could incur substantial costs, including legal fees, and our management may be required to divert a substantial amount of time to an investigation.
To enhance compliance with applicable health care laws, and mitigate potential liability in the event of noncompliance, regulatory authorities, such as the United States Health and Human Services Department Office of Inspector General (“OIG”), have recommended the adoption and implementation of a comprehensive health care compliance program that generally contains the elements of an effective compliance and ethics program described in Section 8B2.1 of the United States Sentencing Commission Guidelines Manual, and for many years the OIG has made available a model compliance program targeted to the clinical laboratory industry. In addition, certain states, such as New York, requires that health care providers, such as clinical laboratories, that engage in substantial business under the state Medicaid program have a compliance program that generally adheres to the standards set forth in the Model Compliance Program. Also, under the Health Care Reform Law,
44
the U.S. Department of Health and Human Services, or HHS, will require suppliers, such as the Company, to adopt, as a condition of Medicare participation, compliance programs that meet a core set of requirements. While we have adopted U.S. healthcare compliance and ethics programs that generally incorporate the OIG’s recommendations, and train our employees in such compliance, having such a program can be no assurance that we will avoid any compliance issues.
Regulations under the 2010 Health Care Reform Legislation are expected to continue being drafted, released and finalized throughout the next several years. Pending the promulgation of these regulations, we are unable to fully evaluate the impact of the 2010 Health Care Reform Legislation.
RISKS RELATED TO INTERNATIONAL OPERATIONS
Failure to obtain regulatory approval outside the U.S. will prevent us from marketing our product candidates abroad.
We intend to market certain of our existing and future product candidates in non-U.S. markets. In order to market our existing and future product candidates in the European Union and many other non-U.S. jurisdictions, we must obtain separate regulatory approvals. We have had limited interactions with non-U.S. regulatory authorities, the approval procedures vary among countries and can involve additional testing, and the time required to obtain approval may differ from that required to obtain FDA approval or clearance. Approval or clearance by the FDA does not ensure approval by regulatory authorities in other countries, and approval by one or more non-U.S. regulatory authority does not ensure approval by other regulatory authorities in other countries or by the FDA. The non-U.S. regulatory approval process may include all of the risks associated with obtaining FDA approval or clearance. We may not obtain non-U.S. regulatory approvals on a timely basis, if at all. We may not be able to file for non-U.S. regulatory approvals and may not receive necessary approvals to commercialize our existing and future product candidates in any market, which would have a material adverse effect on our business, results of operations and financial condition.
Non-U.S. governments often impose strict price controls, which may adversely affect our future profitability.
We intend to seek approval to market certain of our existing and future product candidates in both the U.S. and in non‑U.S. jurisdictions. If we obtain approval in one or more non-U.S. jurisdictions, we will be subject to rules and regulations in those jurisdictions relating to our product. In some countries, particularly countries of the European Union, each of which has developed its own rules and regulations, pricing is subject to governmental control. In these countries, pricing negotiations with governmental authorities can take considerable time after the receipt of marketing approval for a drug or medical device candidate. To obtain reimbursement or pricing approval in some countries, we may be required to conduct a clinical trial that compares the cost-effectiveness of our existing and future product candidates to other available products. If reimbursement of our future product candidates is unavailable or limited in scope or amount, or if pricing is set at unsatisfactory levels, we may be unable to generate revenues and achieve or sustain profitability, which would have a material adverse effect on our business, results of operations and financial condition.
Potential political, economic and military instability in the State of Israel, where we have office, laboratory and manufacturing operations, may adversely affect our results of operations.
We maintain office, laboratory and manufacturing facilities in the State of Israel. Political, economic and military conditions in Israel may directly affect our ability to conduct business. Since the State of Israel was established in 1948, a number of armed conflicts have occurred between Israel and its neighbors. Any hostilities involving Israel or the interruption or curtailment of trade between Israel and its present trading partners, or a significant downturn in the economic or financial condition of Israel, could affect adversely our operations. Ongoing and revived hostilities or other Israeli political or economic factors could harm our operations and product development and cause our revenues to decrease.
Due to the international scope of our business activities, our results of operations may be significantly affected by currency fluctuations.
We derive a significant portion of our consolidated net revenues from international sales, subjecting us to risks relating to fluctuations in currency exchange rates. Currency variations can adversely affect margins on sales of our products in countries outside of the U.S. and margins on sales of products that include components obtained from suppliers located outside of the U.S. Through our subsidiaries, we operate in a wide variety of jurisdictions. Certain countries in which we operate or may operate have experienced geopolitical instability, economic problems and other uncertainties from time to time. To the extent that world events or economic conditions negatively affect our future sales to customers in these and other regions of the world, or the collectability of receivables, our future results of operations, liquidity and financial condition may be adversely affected. Although we do not speculate in the foreign exchange market, we may manage exposures arising in the normal course of business related to fluctuations in foreign currency exchange rates by entering into offsetting positions through the use of foreign exchange forward contracts. Certain firmly committed transactions are hedged with foreign exchange forward
45
contracts whereby exchange rates change, gains and losses on the exposed transactions are partially offset by gains and losses related to the hedging contracts. However, our subsidiaries receive their income and pay their expenses primarily in their local currencies. To the extent that transactions of these subsidiaries are settled in their local currencies, a devaluation of those currencies versus the U.S. dollar could reduce the contribution from these subsidiaries to our consolidated results of operations as reported in U.S. dollars. For financial reporting purposes, such depreciation will negatively affect our reported results of operations since earnings denominated in foreign currencies would be converted to U.S. dollars at a decreased value. While we have employed economic cash flow and fair value hedges to minimize the risks associated with these exchange rate fluctuations, the hedging activities may be ineffective or may not offset more than a portion of the adverse financial impact resulting from currency variations. Accordingly, we cannot assure you that fluctuations in the values of the currencies of countries in which we operate will not materially adversely affect our future results of operations.
We may be exposed to liabilities under the Foreign Corrupt Practices Act, and any determination that we violated the Foreign Corrupt Practices Act could have a material adverse effect on our business.
We are subject to the Foreign Corrupt Practice Act (“FCPA”) and other laws that prohibit U.S. companies or their agents and employees from providing anything of value to a foreign official or political party for the purposes of influencing any act or decision of these individuals in their official capacity to help obtain or retain business, direct business to any person or corporate entity or obtain any unfair advantage. We have operations and agreements with third parties and we generate sales internationally. Our international activities create the risk of unauthorized and illegal payments or offers of payments by our employees, consultants, sales agents or distributors, even though they may not always be subject to our control. We discourage these practices by our employees and agents. However, our existing safeguards and any future improvements may prove to be less than effective, and our employees, consultants, sales agents or distributors may engage in conduct for which we might be held responsible. Any failure by us to adopt appropriate compliance procedures and ensure that our employees and agents comply with the FCPA and applicable laws and regulations in foreign jurisdictions could result in substantial penalties or restrictions on our ability to conduct business in certain foreign jurisdictions.
Violations of the FCPA may result in severe criminal or civil sanctions, and we may be subject to other liabilities, which could negatively affect our business, operating results and financial condition. In addition, the U.S. government may seek to hold our Company liable for successor liability FCPA violations committed by companies in which we invest or that we acquire.
We are subject to risks associated with doing business globally.
Our operations, both within and outside the U.S., are subject to risks inherent in conducting business globally and under the laws, regulations and customs of various jurisdictions and geographies. These risks include fluctuations in currency exchange rates, changes in exchange controls, loss of business in government tenders that are held annually in many cases, nationalization, increasingly complex labor environments, expropriation and other governmental actions, changes in taxation, including legislative changes in U.S. and international taxation of income earned outside of the U.S., importation limitations, export control restrictions, violations of U.S. or local laws, including the FCPA, dependence on a few government entities as customers, pricing restrictions, economic destabilization, political and economic instability, disruption or destruction in a significant geographic region - due to the location of manufacturing facilities, distribution facilities or customers - regardless of cause, including war, terrorism, riot, civil insurrection or social unrest, or natural or man-made disasters, including famine, flood, fire, earthquake, storm or disease. Failure to comply with the laws and regulations that affect our global operations, could have an adverse effect on our business, financial condition or results of operations.
RISKS RELATED TO ACQUISITIONS AND INVESTMENTS
Acquisitions, investments and strategic alliances that we have made or may make in the future may use significant resources, result in disruptions to our business or distractions of our management, may not proceed as planned, and could expose us to unforeseen liabilities. We intend to continue to expand our business through the acquisition of, investments in and strategic alliances with companies, technologies, products, and services. Acquisitions, investments and strategic alliances involve a number of special problems and risks, including, but not limited to:
• |
difficulty integrating acquired technologies, products, services, operations, and personnel with the existing businesses; |
• |
diversion of management’s attention in connection with both negotiating the acquisitions and integrating the businesses; |
• |
strain on managerial and operational resources as management tries to oversee larger operations and investments; |
• |
difficulty implementing and maintaining effective internal control over financial reporting at businesses that we |
46
acquire or invest in, particularly if they are not located near our existing operations;
• |
exposure to unforeseen liabilities of acquired companies or companies in which we invest; |
• |
potential costly and time-consuming litigation, including stockholder lawsuits; |
• |
potential issuance of securities to equity holders of the company being acquired with rights that are superior to the rights of holders of our Common Stock, or which may have a dilutive effect on our stockholders; |
• |
the need to incur additional debt or use cash; and |
• |
the requirement to record potentially significant additional future operating costs for the amortization of intangible assets. |
As a result of these or other problems and risks, businesses we acquire or invest in may not produce the revenues, earnings, or business synergies that we anticipated, and acquired products, services, or technologies might not perform as we expected. As a result, we may incur higher costs and realize lower revenues than we had anticipated. We may not be able to successfully address these problems and we cannot assure you that the acquisitions or investments will be successfully identified and completed or that, if completed, the acquired businesses, investments, products, services, or technologies will generate sufficient revenue to offset the associated costs or other negative effects on our business.
Any of these risks can be greater if an acquisition or investment is large relative to our size. Failure to manage effectively our growth through acquisitions could adversely affect our growth prospects, business, results of operations, financial condition and cash flows.
We may fail to realize the anticipated benefits of the merger with Bio-Reference.
The success of the merger will depend on, among other things, our ability to combine our business with that of Bio-Reference in a manner that facilitates growth opportunities and realizes synergies and cost savings. We believe that the merger will provide an opportunity for revenue growth. However, we must successfully combine our and Bio-Reference’s businesses in a manner that permits these benefits to be realized. In addition, we must achieve the anticipated growth and cost savings without adversely affecting current revenues and investments in future growth. If we are not able to successfully achieve these objectives, the anticipated benefits of the merger may not be realized fully, or at all, or may take longer to realize than expected.
The failure to integrate successfully the business and operations of Bio-Reference in the expected time frame may adversely affect our future results.
Historically, we and Bio-Reference have operated as independent companies. There can be no assurances that our and Bio-Reference’s businesses can be integrated successfully. It is possible that the integration process could result in the loss of our or Bio-Reference’s key employees, the loss of customers, the disruption of either company’s or both companies’ ongoing businesses or in unexpected integration issues, higher than expected integration costs and an overall post-completion integration process that takes longer than originally anticipated. Specifically, the following issues, among others, must be addressed in integrating our operations with Bio-Reference’s operations in order to realize the anticipated benefits of the merger so we perform as expected:
• |
combining the companies’ operations and corporate functions, as well as obtaining anticipated synergies; |
• |
combining our business with Bio-Reference’s business and meeting the capital requirements of the combined company, in a manner that permits us to achieve the cost savings or revenue synergies anticipated to result from the merger, the failure of which would result in the anticipated benefits of the merger not being realized in the time frame currently anticipated or at all; |
• |
integrating the companies’ technologies; |
• |
integrating and unifying the offerings and services available to customers; |
• |
identifying and eliminating redundant and underperforming functions and assets; |
• |
harmonizing and/or addressing differences in the companies’ operating practices, employee development and compensation programs, internal controls and other policies, procedures and processes; |
• |
maintaining existing agreements with customers, distributors, providers and vendors and avoiding delays in entering into new agreements with prospective customers, distributors, providers and vendors; |
• |
addressing possible differences in business backgrounds, corporate cultures and management philosophies; |
• |
consolidating the companies’ administrative and information technology infrastructure; |
47
• |
coordinating distribution and marketing efforts; |
• |
managing the movement of certain positions to different locations; |
• |
coordinating geographically dispersed organizations; and |
• |
effecting actions that may be required in connection with obtaining regulatory approvals. |
In addition, at times the attention of our management and resources may be focused on the integration of the businesses of the two companies and diverted from day-to-day business operations, which may disrupt our ongoing business.
Funding may not be available for us to continue to make acquisitions, investments and strategic alliances in order to grow our business.
We have made and anticipate that we may continue to make acquisitions, investments and strategic alliances with complementary businesses, technologies, products and services to expand our business. Our growth plans rely, in part, on the successful completion of future acquisitions. At any particular time, we may need to raise substantial additional capital or to issue additional equity to finance such acquisitions, investments, and strategic alliances. There is no assurance that we will be able to secure additional funding on acceptable terms, or at all, or obtain the stockholder approvals necessary to issue additional equity to finance such acquisitions, investments, and strategic alliances. If we are unsuccessful in obtaining the financing, our business would be adversely impacted.
We have a large amount of goodwill and other intangible assets as a result of acquisitions and a significant write-down of goodwill and/or other intangible assets would have a material adverse effect on our reported results of operations and net worth.
We have a large amount of goodwill and other intangible assets and we are required to perform an annual, or in certain situations a more frequent, assessment for possible impairment for accounting purposes. At December 31, 2015, we have goodwill and other intangible assets of $2.2 billion, or approximately 78% of our total assets. If we do not achieve our planned operating results, we may be required to incur a non-cash impairment charge. Any impairment charges in the future will adversely affect our results of operations. A significant write down of goodwill and/or other intangible assets would have a material adverse effect on our reported results of operations and net worth.
RISKS RELATED TO OWNERSHIP OF OUR COMMON STOCK
The market price of our Common Stock may fluctuate significantly.
The market price of our Common Stock may fluctuate significantly in response to numerous factors, some of which are beyond our control, such as:
• |
the announcement of new products or product enhancements by us or our competitors; |
• |
results of our clinical trials and other development efforts; |
• |
developments concerning intellectual property rights and regulatory approvals; |
• |
variations in our and our competitors’ results of operations; |
• |
changes in earnings estimates or recommendations by securities analysts, if our Common Stock is covered by analysts; |
• |
developments in the biotechnology, pharmaceutical, diagnostic, and medical device industry; |
• |
the results of product liability or intellectual property lawsuits; |
• |
future issuances of our Common Stock or other securities, including debt; |
• |
purchases and sales of our Common Stock by our officers, directors or affiliates; |
• |
the addition or departure of key personnel; |
• |
announcements by us or our competitors of acquisitions, investments, or strategic alliances; and |
• |
general market conditions and other factors, including factors unrelated to our operating performance. |
Further, the stock market in general, and the market for biotechnology, pharmaceutical, diagnostic, and medical device companies in particular, has experienced extreme price and volume fluctuations in recent years. Continued market fluctuations
48
could result in extreme volatility in the price of our Common Stock, which could cause a decline in the value of our Common Stock.
Directors, executive officers, principal stockholders and affiliated entities own a substantial amount of our capital stock, and they may make decisions that you do not consider to be in the best interests of our stockholders.
As of February 16, 2016, our directors, executive officers, principal stockholders, and affiliated entities beneficially owned, in the aggregate 40.73% of our outstanding voting securities. Frost Gamma Investments Trust (“Gamma Trust”), of which Phillip Frost, M.D., the Company’s Chairman and CEO, is the sole trustee, is deemed to beneficially own in the aggregate approximately 32.8% of our Common Stock as of February 16, 2016. As a result, Dr. Frost acting with other members of management, would have the ability to significantly impact the election of our Board of Directors, the adoption or amendment of provisions in the Company’s Certificate of Incorporation, the approval of mergers and other significant corporate transactions, and the outcome of issues requiring approval by our stockholders. This concentration of ownership may also have the effect of delaying or preventing a change in control of our company that may be favored by other stockholders. This could prevent transactions in which stockholders might otherwise recover a premium for their shares over current market prices.
A significant short position in our stock could have a substantial impact on the trading price of our stock.
Historically, there has been a significant “short” position in our common stock. As of February 12, 2016, investors held a short position of approximately 65,465,949 million shares of our common stock which represented approximately 20.15% of our public float. The anticipated downward pressure on our stock price due to actual or anticipated sales of our stock by some institutions or individuals who engage in short sales of our common stock could cause our stock price to decline. Such stock price decrease could encourage further short-sales that could place additional downward pressure on our stock price. This could lead to further increases in the already large short position in our common stock and cause volatility in our stock price.
The volatility of our stock may cause the value of a stockholder’s investment to decline rapidly. Additionally, if our stock price declines, it may be more difficult for us to raise capital and may have other adverse effects on our business.
Failure to maintain effective internal controls in accordance with Section 404 of the Sarbanes-Oxley Act, including with respect to companies we acquire, could have a material adverse effect on our business and operating results. In addition, current and potential stockholders could lose confidence in our financial reporting, which could have a material adverse effect on the price of our Common Stock.
Section 404 of the Sarbanes-Oxley Act of 2002 requires annual management assessments of the effectiveness of our internal control over financial reporting and a report by our independent registered public accounting firm on the effectiveness of internal control over financial reporting as of year end. We are required to report, among other things, control deficiencies that constitute material weaknesses or changes in internal control that, or that are reasonably likely to, materially affect internal control over financial reporting. A “material weakness” is a significant deficiency or combination of significant deficiencies that results in more than a remote likelihood that a material misstatement of the annual or interim financial statements will not be prevented or detected.
We have identified and remediated control deficiencies in the past, and we cannot assure you that we will at all times in the future be able to report that our internal controls are effective. In addition, material weaknesses in the design and operation of the internal control over financial reporting of companies that we acquire could have a material adverse effect on our business and operating results. Our acquisition of Bio-Reference and possible future acquisitions may increase this risk by expanding the scope and nature of operations over which we must develop and maintain internal control over financial reporting. If we cannot provide reliable financial reports or prevent fraud, our results of operation could be harmed. Our failure to maintain the effective internal control over financial reporting could cause the cost related to remediation to increase and could cause our stock price to decline. In addition, we may not be able to accurately report our financial results, may be subject to regulatory sanction, and investors may lose confidence in our financial statements.
Compliance with changing regulations concerning corporate governance and public disclosure may result in additional expenses.
There have been changing laws, regulations, and standards relating to corporate governance and public disclosure, including the Sarbanes-Oxley Act of 2002, the Dodd-Frank Act, regulations promulgated by the Securities and Exchange Commission and rules promulgated by the NYSE and the other national securities exchanges. These new or changed laws, regulations, and standards are subject to varying interpretations in many cases due to their lack of specificity, and, as a result, their application in practice may evolve over time as new guidance is provided by regulatory and governing bodies, which could result in continuing uncertainty regarding compliance matters and higher costs necessitated by ongoing revisions to
49
disclosure and governance practices. As a result, our efforts to comply with evolving laws, regulations, and standards are likely to continue to result in increased general and administrative expenses and a diversion of management time and attention from revenue-generating activities to compliance activities. Our board members, Chief Executive Officer, Chief Financial Officer, and Principal Accounting Officer could face an increased risk of personal liability in connection with the performance of their duties. As a result, we may have difficulty attracting and retaining qualified board members and executive officers, which could harm our business. If our efforts to comply with new or changed laws, regulations, and standards differ from the activities intended by regulatory or governing bodies, we could be subject to liability under applicable laws or our reputation may be harmed, which could materially adversely affect our business, results of operations and financial condition.
The conversion and redemption features of our 2033 Senior Notes are classified as embedded derivatives and may continue to result in volatility in our financial statements, including having a material impact on our results of operations and the derivative liability recorded.
The conversion rights and redemption options of our 2033 Senior Notes are classified as embedded derivatives and as a result, are marked-to-market to reflect their fair value at each reporting period. The fair value of the embedded derivatives is influenced by a variety of factors, including the actual and anticipated behavior of the holders of the 2033 Senior Notes, the expected volatility of our Common Stock price and our Common Stock price as of the fair value measurement date. Some of these factors are outside of our control. As a result, changes in these factors may have a material impact on our results of operations and the derivative liability recorded in our Consolidated Balance Sheets. Consequently, our financial statements may vary periodically, based on factors other than our revenues and expenses.
ITEM 1B. UNRESOLVED STAFF COMMENTS.
None.
ITEM 2. PROPERTIES.
Our principal corporate office is located at 4400 Biscayne Blvd, Miami, Florida. We lease this space from Frost Real Estate Holdings, LLC (“Frost Real Estate”), an entity which is controlled by Dr. Phillip Frost, our Chairman of the Board and Chief Executive Officer. Pursuant to the lease agreement with Frost Real Estate Holdings, we lease approximately 25,000 square feet, which encompasses space for our corporate offices and administrative services. Effective May 28, 2015, we entered into an amendment to our lease agreement with Frost Real-Estate Holdings. The lease, as amended, is for a five-year term. The lease provides for payments of approximately $66 thousand per month in the first year increasing annually to $75 thousand per month in the fifth year, plus applicable sale tax.
The table below summarizes certain information as to our most significant physical properties as of December 31, 2015:
Location |
Segment and Purpose |
Type of Occupancy |
||
Miami, FL |
Diagnostics & Pharmaceutical: Corporate Headquarters |
Leased |
||
Elmwood Park, NJ |
Diagnostics: Main Laboratory |
Leased |
||
Gaithersburg, MD |
Diagnostics: Genetics Laboratory |
Leased |
||
Nes Ziona, Israel |
Pharmaceutical: Research and Development, CTP |
Leased |
||
Woburn, MA |
Diagnostics |
Leased |
||
Nesher, Israel |
Pharmaceuticals: API Manufacturing |
Leased |
||
Guadalajara, Mexico |
Pharmaceuticals: Pharmaceutical Manufacturing |
Owned |
||
Banyoles, Spain |
Pharmaceuticals: Pharmaceutical Manufacturing |
Owned |
||
Barcelona, Spain |
Pharmaceuticals: Research and Development |
Leased |
||
Waterford, Ireland |
Pharmaceuticals: Pharmaceutical Manufacturing |
Leased |
||
Santiago, Chile |
Pharmaceuticals: Office; Warehouse |
Leased |
||
ITEM 3. LEGAL PROCEEDINGS.
Following the announcement of entry into an agreement and plan of merger with Bio-Reference, four putative class action complaints challenging the merger were filed in the Superior Court of New Jersey in Bergen County (the “Court”). The parties subsequently executed a stipulated consent order that the actions would be consolidated for all purposes, including trial,
50
in the Chancery Division under Docket No. C-207-15, bearing the caption In re Bio-Reference Laboratories, Inc. Shareholder Litigation. The complaints name Bio-Reference, OPKO, a wholly-owned merger subsidiary of OPKO (“Merger Sub”) and members of the Bio-Reference board as defendants. The complaints generally allege, among other things, that members of the Bio-Reference board breached their fiduciary duties to Bio-Reference’s shareholders by agreeing to sell Bio-Reference for an inadequate price and agreeing to inappropriate deal protection provisions in the merger agreement that may preclude Bio-Reference from soliciting any potential acquirers and limit the ability of the Bio-Reference board to act with respect to investigating and pursuing superior proposals and alternatives. The complaints also allege that Bio-Reference, OPKO and Merger Sub have aided and abetted the Bio-Reference board members’ breaches of their fiduciary duties. In August, the parties executed a memorandum of understanding reflecting terms of a settlement, which was replaced in September 2015 by a stipulation and agreement of compromise, settlement and release resolving all matters between them. In January 2016, the Court entered an order finally approving the settlement. The settlement did not have a material impact on our business, financial condition, results of operations or cash flows.
On December 18, 2013, Bio-Reference filed an action in the Superior Court of New Jersey against Horizon Blue Cross Blue Shield of New Jersey (“Horizon”), captioned Bio-Reference Laboratories, Inc. v. Horizon Healthcare Services, Inc. d/b/a Horizon Blue Cross Blue Shield of New Jersey, Docket No. BER L-009748-13 (N.J. Super. Ct. Bergen Cnty.). Bio-Reference has been an in-network provider to Horizon’s preferred provider organization (“PPO”) members for more than 20 years and filed the lawsuit after attempts to resolve its dispute with Horizon were unsuccessful.
Bio-Reference currently provides services to Horizon pursuant to an Ancillary Services Provider Agreement entered into in 2003 and amended in 2007. The central claims in the lawsuit arise from Bio-Reference’s performance of laboratory services since at least 2008 for members of Horizon’s NJ DIRECT plan, who receive benefits under a program that Horizon has bid, promoted, and represented to be a PPO product for New Jersey state, county, and municipal workers and teachers. The lawsuit alleges that, despite these representations, Horizon has been improperly treating NJ DIRECT as a Managed Care program in its dealings with Bio-Reference, thereby costing Bio-Reference more than $20,000,000 in unreimbursed services and depriving state beneficiaries of valuable rights and benefits to which they are entitled. The lawsuit alleges that Horizon furthered its fraud against Bio-Reference by means of a sham Request for Proposal issued in 2011 and through false and incorrect communications to Bio-Reference and other providers. Bio-Reference asserts claims for breach of contract, breach of the implied covenant of good faith and fair dealing, and fraud against Horizon. In addition to compensatory damages, Bio-Reference seeks to recover punitive damages from Horizon due to Horizon’s intentional and malicious misconduct. Bio-Reference also seeks declaratory and injunctive relief.
Bio-Reference and Horizon have completed discovery, and Horizon has filed a motion for summary judgment, which Bio-Reference is opposing, and which will be argued before the Court on March 18, 2016. Trial in the matter is currently set for April 2016. Bio-Reference intends to vigorously prosecute its claims against Horizon.
ITEM 4. MINE SAFETY DISCLOSURES.
Not applicable.
51
PART II
ITEM 5. MARKET FOR REGISTRANT’S COMMON EQUITY, RELATED STOCKHOLDER MATTERS
AND ISSUER PURCHASES OF EQUITY SECURITIES.
Our Common Stock is traded publicly on the New York Stock Exchange (“NYSE”) and the Tel Aviv Stock Exchange under the symbol “OPK”.
The following table sets forth for the periods indicated the high and low sales prices per share of our Common Stock during each of the quarters set forth below as reported on the NYSE:
High |
Low |
||||||
2015 |
|||||||
First Quarter |
$ |
15.23 |
$ |
9.81 |
|||
Second Quarter |
19.20 |
13.71 |
|||||
Third Quarter |
17.51 |
8.23 |
|||||
Fourth Quarter |
11.49 |
8.20 |
|||||
2014 |
|||||||
First Quarter |
$ |
10.25 |
$ |
7.32 |
|||
Second Quarter |
9.83 |
7.82 |
|||||
Third Quarter |
9.62 |
8.09 |
|||||
Fourth Quarter |
10.16 |
8.02 |
|||||
As of February 16, 2016, there were approximately 628 holders of record of our Common Stock.
We have not declared or paid any cash dividends on our Common Stock. No cash dividends have been previously paid on our Common Stock and none are anticipated in fiscal 2016.
Stock Performance Graph
The following graph compares the five-year cumulative total return of our Common Stock with the S&P 500 Index and the NASDAQ Biotechnology Index. The graph assumes $100 invested on December 31, 2010 in our Common Stock and in each of the foregoing indices. The stock price performance reflected in the graph below is not necessarily indicative of future price performance.
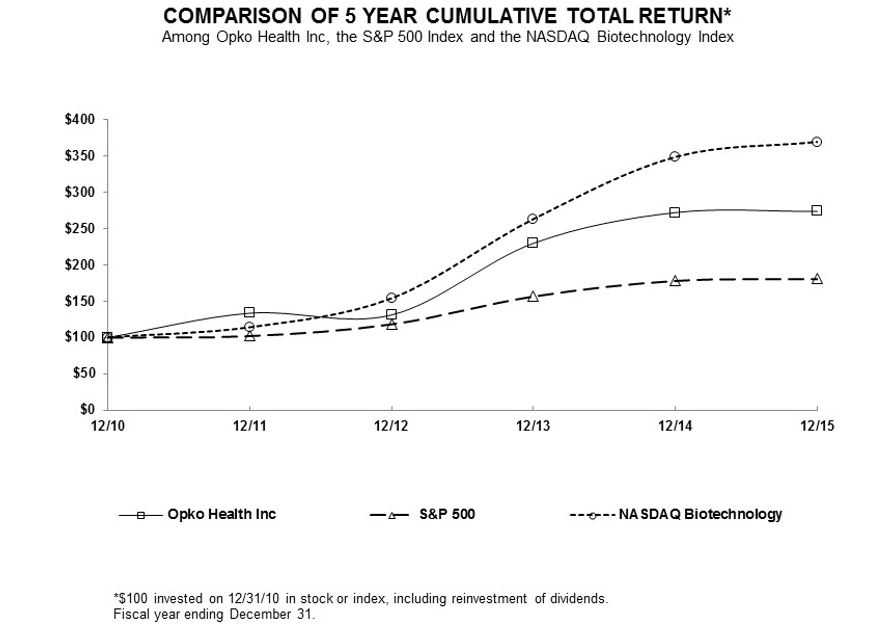
12/31/2010 |
12/31/2011 |
12/31/2012 |
12/31/2013 |
12/31/2014 |
12/31/2015 |
||||||||||||||||||
OPKO Health, Inc. |
$ |
100.00 |
$ |
133.51 |
$ |
131.06 |
$ |
229.97 |
$ |
272.21 |
$ |
273.84 |
|||||||||||
S&P 500 |
100.00 |
102.11 |
118.45 |
156.82 |
178.29 |
180.75 |
|||||||||||||||||
NASDAQ Biotechnology |
100.00 |
113.92 |
153.97 |
263.29 |
348.49 |
369.06 |
|||||||||||||||||
Recent Sales of Unregistered Securities
None.
53
ITEM 6. SELECTED FINANCIAL DATA.
The following selected historical consolidated statement of operations data for the years ended December 31, 2015, 2014, 2013, 2012, and 2011 and the consolidated balance sheet data as of December 31, 2015, 2014, 2013, 2012, and 2011, below are derived from our audited consolidated financial statements and related notes thereto. This data should be read in conjunction with our “Management’s Discussion and Analysis of Financial Condition and Results of Operation” and our consolidated financial statements and the related notes thereto.
For the years ended December 31, |
||||||||||||||||||||
(In thousands, except share and per share information) |
2015 |
2014 |
2013 |
2012 |
2011 |
|||||||||||||||
Statement of operations data: |
||||||||||||||||||||
Revenues |
$ |
491,738 |
$ |
91,125 |
$ |
96,530 |
$ |
47,044 |
$ |
27,979 |
||||||||||
Costs and expenses: |
||||||||||||||||||||
Cost of revenue |
235,239 |
48,009 |
48,860 |
27,878 |
17,243 |
|||||||||||||||
Operating expenses |
354,980 |
188,931 |
127,302 |
56,435 |
33,925 |
|||||||||||||||
Total costs and expenses |
590,219 |
236,940 |
176,162 |
84,313 |
51,168 |
|||||||||||||||
Operating loss from continuing operations |
(98,481 |
) |
(145,815 |
) |
(79,632 |
) |
(37,269 |
) |
(23,189 |
) |
||||||||||
Other income and (expense), net |
(39,517 |
) |
(25,212 |
) |
(24,586 |
) |
165 |
(1,044 |
) |
|||||||||||
Income tax benefit (provision) |
113,675 |
(24 |
) |
(1,672 |
) |
9,626 |
19,358 |
|||||||||||||
Loss from continuing operations |
(31,428 |
) |
(174,638 |
) |
(117,346 |
) |
(29,540 |
) |
(6,464 |
) |
||||||||||
Net loss attributable to common shareholders |
$ |
(30,028 |
) |
$ |
(171,666 |
) |
$ |
(114,827 |
) |
$ |
(31,288 |
) |
$ |
(3,662 |
) |
|||||
Loss per share, basic and diluted: |
||||||||||||||||||||
Loss from continuing operations |
$ |
(0.06 |
) |
$ |
(0.41 |
) |
$ |
(0.32 |
) |
$ |
(0.11 |
) |
$ |
(0.03 |
) |
|||||
Weighted average number of common shares outstanding basic and diluted: |
488,065,908 |
422,014,039 |
355,095,701 |
295,750,077 |
280,673,122 |
|||||||||||||||
Balance sheet data: |
||||||||||||||||||||
Total assets |
$ |
2,799,614 |
$ |
1,267,664 |
$ |
1,391,516 |
$ |
289,830 |
$ |
229,489 |
||||||||||
Long-term liabilities |
$ |
567,918 |
$ |
348,812 |
$ |
426,687 |
$ |
34,168 |
$ |
25,443 |
||||||||||
Series D Preferred Stock |
$ |
— |
$ |
— |
$ |
— |
$ |
24,386 |
$ |
24,386 |
||||||||||
Total shareholders’ equity |
$ |
1,979,794 |
$ |
835,741 |
$ |
872,979 |
$ |
178,894 |
$ |
160,882 |
||||||||||
54
ITEM 7. MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS.
This Annual Report on Form 10-K contains certain forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995 (“PSLRA”), Section 27A of the Securities Act of 1933, as amended, (the “Securities Act”), and Section 21E of the Securities Exchange Act of 1934, as amended, (the “Exchange Act”), about our expectations, beliefs, or intentions regarding our product development efforts, business, financial condition, results of operations, strategies, or prospects. You can identify forward-looking statements by the fact that these statements do not relate strictly to historical or current matters. Rather, forward-looking statements relate to anticipated or expected events, activities, trends, or results as of the date they are made. Because forward-looking statements relate to matters that have not yet occurred, these statements are inherently subject to risks and uncertainties that could cause our actual results to differ materially from any future results expressed or implied by the forward-looking statements. Many factors could cause our actual activities or results to differ materially from the activities and results anticipated in forward-looking statements. These factors include those contained in “Item 1A — Risk Factors” of this Annual Report on Form 10-K. We do not undertake any obligation to update forward-looking statements. We intend that all forward-looking statements be subject to the safe harbor provisions of PSLRA. These forward-looking statements are only predictions and reflect our views as of the date they are made with respect to future events and financial performance.
OVERVIEW
We are a diversified healthcare company that seeks to establish industry-leading positions in large and rapidly growing medical markets. Our diagnostics business includes Bio-Reference Laboratories, the nation’s third-largest clinical laboratory with a core genetic testing business and a 420-person salesforce to drive growth and leverage new products, including the 4Kscore prostate cancer test and the Claros1 in-office immunoassay platform. Our pharmaceutical operations feature Rayaldee, a treatment for secondary hyperparathyroidism (“SHPT”) in patients with stage 3 or 4 chronic kidney disease (“CKD”) and vitamin D insufficiency (March 29, 2016 PDUFA date) and VARUBI™ for chemotherapy-induced nausea and vomiting (launched by partner TESARO in November 2015). Our pharmaceutical business includes OPKO Biologics, which features hGH-CTP, a once-weekly human growth hormone injection (in Phase 3 and partnered with Pfizer), and a once-daily Factor VIIa drug for hemophilia (Phase 2a).
We operate established pharmaceutical platforms in Spain, Ireland, Chile and Mexico, which are generating revenue and from which we expect to generate positive cash flow and facilitate future market entry for our products currently in development. EirGen, our specialty pharmaceutical manufacturing and development site in Ireland, is focused on the development and commercial supply of high potency, high barrier to entry pharmaceutical products. In addition, we operate a specialty active pharmaceutical ingredients (“APIs”) manufacturer in Israel, which we expect will facilitate the development of our pipeline of molecules and compounds for our proprietary products.
RECENT DEVELOPMENTS
In August 2015, we completed the acquisition of Bio-Reference, the third largest full service clinical laboratory in the United States, known for its innovative technological solutions and pioneering leadership in the areas of genomics and genetic sequencing. Holders of Bio-Reference common stock received 76,566,147 shares of OPKO Common Stock for the outstanding shares of Bio-Reference common stock. The transaction was valued at approximately $950.1 million, based on a closing price per share of our Common Stock of $12.38 as reported by the New York Stock Exchange on the closing date, or $34.05 per share of Bio-Reference common stock. Included in the transaction value is $2.3 million related to the value of replacement stock option awards attributable to pre-merger service.
In May 2015, we entered into a series of purchase agreements to acquire all of the issued and outstanding shares of EirGen, a specialty pharmaceutical company incorporated in Ireland focused on the development and commercial supply of high potency, high barrier to entry pharmaceutical products, for $133.8 million in the aggregate. We acquired the outstanding shares of EirGen for approximately $100.2 million in cash and delivered 2,420,487 shares of our Common Stock valued at approximately $33.6 million based on the closing price per share of our Common Stock as reported by the New York Stock Exchange on the closing date of the acquisition, $13.88 per share.
TESARO’s NDA for approval of oral VARUBI™, an investigational neurokinin-1 receptor antagonist in development for the prevention of chemotherapy-induced nausea and vomiting, was approved by the U.S. FDA in September 2015, and in November 2015, TESARO announced the commercial launch of VARUBI™ in the United States. Under the terms of the TESARO license, TESARO is obligated to pay us tiered royalties on annual net sales of licensed products achieved in the
55
United States and Europe at percentage rates that range from the low double digits to the low twenties, and outside of the United States and Europe at low double-digit percentage rates.
We have been granted a Category I CPT code by the AMA for our 4Kscore test, which will be published in August 2016 and effective January 1, 2017. This upgrades the 4Kscore test from a Category III Administrative code to a Category I CPT code, a designation reserved for established diagnostic tests. CPT codes are used by insurance companies and government payers to describe health care services and procedures, and having a Category I CPT code is critical to facilitate reimbursement in government programs such as Medicare and Medicaid, as well as private insurance programs. We believe having the Category I CPT code will help facilitate obtaining broader coverage from payers for the 4Kscore test and allow greater access to the test for a broader group of patients across the U.S.
RESULTS OF OPERATIONS
For The Years Ended December 31, 2015 and December 31, 2014
Revenues. Revenues for the year ended December 31, 2015 increased $400.6 million compared to the prior year. Our acquisition of Bio-Reference in August 2015 accounted for $321.9 million of the year-over-year revenue growth. Revenues for the years ended December 31, 2015 and 2014 were as follows:
Revenues |
For the year ended December 31, |
||||||||||
(In thousands) |
2015 |
2014 |
Change |
||||||||
Revenue from services |
$ |
329,739 |
$ |
8,666 |
$ |
321,073 |
|||||
Revenue from products |
80,146 |
76,983 |
3,163 |
||||||||
Revenue from transfer of intellectual property and other |
81,853 |
5,476 |
76,377 |
||||||||
Total revenues |
$ |
491,738 |
$ |
91,125 |
$ |
400,613 |
|||||
The increase in Revenue from services is attributable to the acquisition of Bio-Reference in August 2015. The increase in Revenue from products principally reflects $12.1 million of revenue from EirGen, which we acquired in May 2015, which was partially offset by the unfavorable impact of foreign exchange rates of approximately $8.7 million, and decreased revenue from SciVac Therapeutics Inc. (“STI”), a VIE we deconsolidated in July 2015. The increase in Revenue from transfer of intellectual property principally reflects $65.5 million of revenue from the transfer of intellectual property related to the Pfizer Transaction and $15.0 million of revenue from a milestone payment from our licensee TESARO in the fourth quarter of 2015 compared to $5.0 million of revenue from a milestone payment from our licensee TESARO in 2014. We are recognizing the non-refundable $295.0 million upfront payments received in the Pfizer Transaction on a straight-line basis over the expected performance period. The performance period is expected to continue through 2019, when we anticipate completing the various research and development services that are specified in the Pfizer Transaction.
Costs of revenue. Costs of revenue for the year ended December 31, 2015 increased $187.2 million compared to the prior year. Our acquisition of Bio-Reference in August 2015 accounted for $183.3 million of the year-over-year cost of revenue growth. Cost of revenue for the years ended December 31, 2015 and 2014 were as follows:
Cost of Revenue |
For the year ended December 31, |
||||||||||
(In thousands) |
2015 |
2014 |
Change |
||||||||
Cost of service revenue |
$ |
193,305 |
$ |
9,372 |
$ |
183,933 |
|||||
Cost of product revenue |
41,934 |
38,637 |
3,297 |
||||||||
Total cost of revenue |
$ |
235,239 |
$ |
48,009 |
$ |
187,230 |
|||||
The increase in cost of service revenue is attributable to the acquisition of Bio-Reference in August 2015. The increase in cost of product revenue principally reflects cost of revenue of $6.8 million from EirGen, which we acquired in May 2015, which was partially offset by the impact of foreign exchange rates of approximately $5.2 million and the deconsolidation of STI in July 2015.
Selling, general and administrative expenses. Selling, general and administrative expenses for the years ended December 31, 2015 and 2014 were $196.6 million and $57.9 million, respectively. The increase in selling, general and administrative expenses for the year ended December 31, 2015 was primarily due to the acquisitions of Bio-Reference and EirGen in 2015,
56
which recognized $118.1 million and $1.8 million of selling, general and administrative expenses in 2015, respectively, increased personnel expenses as we expand our sales, marketing and administrative staff and add infrastructure, and an increase in professional fees attributable to our acquisitions of Bio-Reference and EirGen. Selling, general and administrative expenses during the years ended December 31, 2015 and 2014, include bad debt expense of $24.6 million and $0.7 million, respectively, and equity-based compensation expense of $17.4 million and $9.7 million, respectively. The increase in bad debt expense is due to the acquisition of Bio-Reference. The increase in equity-based compensation expense is due to additional options grants made in 2015 and fluctuations in the price of our common stock.
Research and development expenses. Research and development expenses for the years ended December 31, 2015 and 2014 were $99.5 million and $83.6 million, respectively. Research and development costs include external and internal expenses, partially offset by third-party grants and funding arising from collaboration agreements. External expenses include clinical and non-clinical activities performed by contract research organizations, lab services, purchases of drug and diagnostic product materials and manufacturing development costs. We track external research and development expenses by individual program for phase 3 clinical trials for drug approval and PMA’s (pre-market approval) for diagnostics tests, if any. Internal expenses include employee-related expenses including salaries, benefits and stock-based compensation expense. Other internal research and development expenses are incurred to support overall research and development activities and include expenses related to general overhead and facilities.
The following table summarizes the components of our research and development expenses:
For the years ended December 31, |
|||||||
2015 |
2014 |
||||||
External expenses: |
|||||||
Phase 3 clinical trials |
$ |
12,178 |
$ |
14,512 |
|||
Manufacturing expense for biological products |
22,674 |
18,692 |
|||||
Earlier-stage programs |
6,900 |
9,093 |
|||||
Research and development employee-related expenses |
27,363 |
21,642 |
|||||
Other internal research and development expenses |
32,689 |
21,982 |
|||||
Third-party grants and funding from collaboration agreements |
(2,316 |
) |
(2,350 |
) |
|||
Total research and development expenses |
$ |
99,488 |
$ |
83,571 |
|||
The increase in research and development expenses during the year ended December 31, 2015, is primarily due to a $16.7 million increase in research and development expenses related to hGH-CTP, a long acting human growth hormone which was outlicensed to Pfizer in 2015, including manufacturing expense for biological products, and the recognition of $2.3 million of expense for our NDA submission to the FDA for oral Rayaldee in May 2015. Research and development expenses for the year ended December 31, 2015 also include $4.1 million from the acquisitions of Bio-Reference and EirGen in August 2015 and May 2015, respectively. This was partially offset by decreased expenses incurred by OPKO Renal related to phase 3 clinical trials for Rayaldee, which were completed in 2014. In addition, during the year ended December 31, 2015 and 2014, we recorded, as an offset to research and development expenses, $2.3 million and $2.4 million, respectively, related to research and development grants received from our collaboration and funding agreements. Research and development expenses for the year ended December 31, 2015 and 2014 include equity-based compensation expense of $7.9 million and $5.0 million, respectively. We expect our research and development expense to increase as we continue to expand our research and development of potential future products.
In-Process Research and Development. In May 2014, we acquired Inspiro in a stock for stock transaction. We recorded the transaction as an asset acquisition and recorded the assets and liabilities at fair value, and as a result, we recorded $10.1 million of acquired in-process research and development expense. In addition, pursuant to our agreement with Merck & Co. (“Merck”), we were required to make a $2.0 million payment upon the achievement of a milestone for VARUBI™ which was achieved in the fourth quarter of 2014. The agreement was accounted for as an asset acquisition and the entire $2.0 million milestone payment was allocated to in-process research and development expense. No In-process research and development expense was incurred during the year ended December 31, 2015.
Contingent consideration. Contingent consideration expenses for the years ended December 31, 2015 and 2014, were $5.0 million and $24.4 million, respectively. The decrease in contingent consideration expense was attributable to OPKO Renal resulting from an increase in the fair value of our contingent obligations to OPKO Renal in 2014 due to changes in assumptions regarding probabilities of successful achievement of future milestones driven by the two successful phase 3 trials of Rayaldee in 2014. The contingent consideration liabilities at December 31, 2015 relate to potential amounts payable to
57
former stockholders of CURNA, OPKO Diagnostics, OPKO Health Europe and OPKO Renal pursuant to our acquisition agreements in January 2011, October 2011, August 2012 and March 2013, respectively.
Amortization of intangible assets. Amortization of intangible assets was $28.0 million and $10.9 million, respectively, for the years ended December 31, 2015 and 2014. Amortization expense reflects the amortization of acquired intangible assets with defined useful lives. Amortization of intangible assets for the year ended December 31, 2015 includes $14.6 million and $1.7 million from Bio-Reference and EirGen which we acquired in August 2015 and May 2015, respectively. Our IPR&D assets will not be amortized until the underlying development programs are completed. Upon obtaining regulatory approval by the U.S. FDA, the IPR&D assets will then be accounted for as a finite-lived intangible asset and amortized on a straight-line basis over its estimated useful life.
Grant repayment. During the year ended December 31, 2015, we made a payment of $25.9 million to the Office of the Chief Scientist of the Israeli Ministry of Economy (“OCS”) in connection with repayment obligations resulting from grants previously made by the OCS to OPKO Biologics to support development of hGH-CTP and the outlicense of the technology outside of Israel.
Interest income. Interest income for the years ended December 31, 2015 and 2014, was not significant as our cash investment strategy emphasizes the security of the principal invested and fulfillment of liquidity needs.
Interest expense. Interest expense for the years ended December 31, 2015 and 2014, was $8.4 million and $12.3 million, respectively. Interest expense is principally related to interest incurred on the 2033 Senior Notes and the amortization of related deferred financing costs. The decrease in interest expense for the year ended December 31, 2015 compared to 2014 is due to a decrease in the principal amount of 2033 Senior Notes outstanding from $87.6 million at December 31, 2014 to $32.2 million as of December 31, 2015. This was partially offset by interest expense of $1.9 million from Bio-Reference due to outstanding debt under their credit facility. Interest expense for the years ended December 31, 2015 and 2014 also reflect non-cash write-offs of deferred financing costs of $1.0 million and $1.5 million as interest expense related to exchange or conversion of $55.4 million and $70.4 million principal of 2033 Senior Notes during the years ended December 31, 2015 and 2014, respectively.
Fair value changes of derivative instruments, net. Fair value changes of derivative instruments, net for the years ended December 31, 2015 and 2014, were $39.1 million and $10.6 million of expense, respectively. Fair value changes of derivative instruments, net principally related to non-cash expense related to the changes in the fair value of the embedded derivatives in the 2033 Senior Notes of $36.6 million and $12.2 million for the years ended December 31, 2015 and 2014, respectively.
Other income and (expense), net. Other income and (expense), net for the years ended December 31, 2015 and 2014, were $7.7 million of income and $(3.1) million of expense, respectively. The increase in other income and (expense), net for the year ended December 31, 2015 compared to 2014 is primarily due to a $15.9 million gain recognized on the deconsolidation of STI in the third quarter of 2015. This was partially offset by a $7.3 million other-than-temporary impairment charge to write our investment in RXi Pharmaceuticals Corporation down to its fair value of $0.9 million as of December 31, 2015 compared to a $1.4 million other-than-temporary impairment charge to our investment in ARNO Therapeutics in 2014.
Income tax benefit (provision). Our income tax benefit is due to a $93.4 million release of OPKO’s valuation allowance on our U.S. deferred tax assets as a result of the merger with Bio-Reference. This was partially offset by expense recognized on taxable income from the Pfizer Transaction during the year ended December 31, 2015. In addition, our income tax benefit (provision) reflects the projected income tax payable in the U.S., Ireland, Israel, Chile, Spain, Mexico, and Luxembourg.
Loss from investments in investees. We have made investments in other early stage companies that we perceive to have valuable proprietary technology and significant potential to create value for us as a shareholder or member. We account for these investments under the equity method of accounting, resulting in the recording of our proportionate share of their losses until our share of their loss exceeds our investment. Until the investees’ technologies are commercialized, if ever, we anticipate they will continue to report a net loss. Loss from investments in investees was $7.1 million and $3.6 million for the years ended December 31, 2015 and 2014, respectively. In the third quarter of 2015 we deconsolidated STI, and account for our retained interest in STI as an equity method investment.
For The Years Ended December 31, 2014 and December 31, 2013
Revenues. Revenues for the year ended December 31, 2014, were $91.1 million, compared to $96.5 million for the year ended December 31, 2013. The decrease in revenue principally reflects non-recurring, non-cash revenue related to the transfer of technology under the RXi Asset Purchase Agreement of $12.5 million in 2013, which was partially offset by (i) a milestone payment of $5.0 million from TESARO during the year ended December 31, 2014, which we recognized in Revenue from transfer of intellectual property and (ii) a 14% increase in pharmaceutical product revenue principally from FineTech of $6.2
58
million for the year ended December 31, 2014. In addition, pharmaceutical product revenue from our European and Mexican operations increased by $2.5 million and $1.6 million, respectively, during the year ended December 31, 2014, primarily due to increased sales by OPKO Health Europe and an increase in government tenders in Mexico. Revenue related to OPKO Lab decreased $2.9 million during the year ended December 31, 2014, compared to the year ended December 31, 2013, primarily related to decreased reimbursement rates from government payors and decreased specimen volume, partially offset by revenue from the launch of our 4Kscore test and a price increase to non-government payors initiated in June 2014.
Costs of revenue. Costs of revenue for the year ended December 31, 2014, were $48.0 million, compared to $48.9 million for the year ended December 31, 2013. Costs of revenue for the year ended December 31, 2014 decreased principally due to decreased revenue at OPKO Lab, which has a lower margin than pharmaceutical product sales. In addition, inventory obsolescence charges decreased $0.9 million for the year ended December 31, 2014 compared to 2013. This was partially offset by increased cost of revenue due to increased pharmaceutical product sales.
Selling, general and administrative expenses. Selling, general and administrative expenses for the year ended December 31, 2014 were $57.9 million, compared to $55.3 million for the year ended December 31, 2013. The increase in selling, general and administrative expenses for the year ended December 31, 2014 was a result of increased personnel expenses including equity based compensation as well as sales and marketing activities related to the launch of our 4Kscore test in the U.S. in March 2014 and Europe in September 2014. These increases were partially offset by decreased professional fees as the 2013 period included expenses related to the acquisitions of OPKO Renal and OPKO Biologics. Selling, general and administrative expenses during the years ended December 31, 2014 and 2013, include equity-based compensation expense of $9.7 million and $7.3 million, respectively.
Research and development expenses. Research and development expenses for the year ended December 31, 2014 were $83.6 million, compared to $53.9 million for the year ended December 31, 2013. Research and development costs include external and internal expenses, partially offset by third-party grants and funding arising from collaboration agreements. External expenses include clinical and non-clinical activities performed by contract research organizations, lab services, purchases of drug and diagnostic product materials and manufacturing development costs. We track external research and development expenses by individual program for phase 3 clinical trials for drug approval and PMA’s (pre-market approval) for diagnostics tests, if any. Internal expenses include employee-related expenses including salaries, benefits and stock-based compensation expense. Other internal research and development expenses are incurred to support overall research and development activities and include expenses related to general overhead and facilities.
The following table summarizes the components of our research and development expenses:
For the years ended December 31, |
|||||||
2014 |
2013 |
||||||
External expenses: |
|||||||
Phase 3 clinical trials |
$ |
14,512 |
$ |
13,078 |
|||
CMC expense for biological products |
18,692 |
1,765 |
|||||
Earlier-stage programs |
9,093 |
4,599 |
|||||
Research and development employee-related expenses |
21,642 |
17,215 |
|||||
Other internal research and development expenses |
21,982 |
18,998 |
|||||
Third-party grants and funding from collaboration agreements |
(2,350 |
) |
(1,753 |
) |
|||
Total research and development expenses |
$ |
83,571 |
$ |
53,902 |
|||
The increase in research and development expenses during the year ended December 31, 2014, as compared to the year ended December 31, 2013, principally resulted from $38.6 million of costs related to OPKO Biologics which we acquired in August 2013 and an increase related to research and development expenses incurred by OPKO Renal related to the external costs of two pivotal phase 3 clinical trials for Rayaldee which were completed in 2014, and a third open-label phase 3 trial completed in 2015. OPKO Biologics principally incurred development and clinical manufacturing costs (“CMC”) related to hGH-CTP, a long acting human growth hormone which was outlicensed to Pfizer in 2015. Research and development expenses for the years ended December 31, 2014 and 2013 include equity-based compensation expense of $5.0 million and $3.6 million, respectively. Research and development expenses for the year ended December 31, 2013, includes an offset to research and development expenses of $2.7 million related to the correction of an error related to equity awards granted to non-employees with performance based vesting.
Contingent consideration. Contingent consideration expenses for the years ended December 31, 2014 and 2013, were $24.4 million and $6.9 million, respectively. The increase in contingent consideration expense was primarily attributable to an
59
increase in the fair value of our contingent obligations to the former stockholders of OPKO Renal due to changes in assumptions regarding probabilities of successful achievement of future milestones driven by the two successful phase 3 trials of Rayaldee in 2014. The contingent consideration liabilities at December 31, 2014 relate to potential amounts payable to former stockholders of CURNA, OPKO Diagnostics, OPKO Health Europe and OPKO Renal pursuant to our acquisition agreements in January 2011, October 2011, August 2012 and March 2013, respectively.
Amortization of intangible assets. Amortization of intangible assets was $10.9 million and $11.1 million, respectively, for the years ended December 31, 2014 and 2013. Amortization expense reflects the amortization of acquired intangible assets with defined useful lives. The acquisitions of OPKO Renal and OPKO Biologics resulted in principally acquiring IPR&D assets which will not be amortized until the underlying development programs are completed. Upon obtaining regulatory approval by the FDA, the IPR&D asset will then be accounted for as a finite-lived intangible asset and amortized on a straight-line basis over its estimated useful life.
In-Process Research and Development. In May 2014, we acquired Inspiro, a privately held company that is developing the Inspiromatic, a “smart” easy-to-use dry powder inhaler with several advantages over existing devices. We recorded the transaction as an asset acquisition and recorded the assets and liabilities at fair value. As the asset had no alternative future use, we recorded $10.1 million of acquired in-process research and development expense. In addition, pursuant to our agreement with Merck, we were required to make a $2.0 million payment upon the achievement of a milestone for rolapitant which was achieved in the fourth quarter of 2014. The agreement was accounted for as an asset acquisition and the entire $2.0 million milestone payment was allocated to in-process research and development expense. We did not have any such activity during the year ended December 31, 2013.
We record expense for in-process research and development projects accounted for as asset acquisitions which have not reached technological feasibility and which have no alternative future use. Inspiromatic and rolapitant have not reached a stage of technological feasibility and have no alternative future use.
Other income and (expense), net. Other income and (expense), net for the years ended December 31, 2014 and 2013 was ($25.2) million and $24.6 million of expense, respectively. During the year ended December 31, 2014, we recorded $12.2 million non-cash other charge, net, related to the changes in the fair value of the embedded derivatives in the 2033 Senior Notes, and a $2.7 million gain as the result of the exchange of $70.4 million principal of 2033 Senior Notes in June 2014. Other income and (expense), net, for the year ended December 31, 2014, also included $12.3 million of interest expense principally related to interest incurred on the 2033 Senior Notes and the amortization of related deferred financing costs. Other income and (expense), net for the year ended December 31, 2014, includes a $1.4 million other-than-temporary impairment charge to write our investment in ARNO Therapeutics down to its fair value of $0.6 million as of December 31, 2014.
For the year ended December 31, 2013, we recorded a $52.7 million non-cash charge, net, related to the changes in the fair value of the embedded derivatives in the 2033 Senior Notes, partially offset by a $1.0 million gain on early partial conversion of the 2033 Senior Notes, income of $6.5 million related to changes in the fair value of the Pharmsynthez Note Receivable, a certain Pharmsynthez purchase option, warrants and options received in connection with our investment in Neovasc and ARNO, and by a gain of $29.9 million on the sale of certain of our strategic investments. Other income and (expense), net, for the year ended December 31, 2013, also included $13.8 million of interest expense primarily related to the 2033 Senior Notes and the amortization of related deferred financing costs. The decrease in interest expense for the year ended December 31, 2014 compared to the same period in 2013 is due to the exchange of $70.4 million principal of 2033 Senior Notes in June 2014, which was partially offset by a non-cash write-off of deferred financing costs of $1.5 million as interest expense related to exchange of the 2033 Senior Notes in June 2014.
Income tax benefit (provision). Our income tax provision reflects the projected income tax payable in Israel, Chile, Spain, Mexico, Canada and SciVac Ltd, a consolidated variable interest entity. We have recorded a full valuation allowance against our deferred tax assets in the U.S.
Loss from investments in investees. We have made investments in other early stage companies that we perceive to have valuable proprietary technology and significant potential to create value for us as a shareholder. We account for these investments under the equity method of accounting, resulting in the recording of our proportionate share of their losses until our share of their loss exceeds our investment. Until the investees’ technologies are commercialized, if ever, we anticipate they will continue to report a net loss. Loss from investments in investees was $3.6 million and $11.5 million for the years ended December 31, 2014 and 2013, respectively. The decrease in loss from investments in investees is primarily due to decreased losses at RXi Pharmaceuticals Corporation and Cocrystal Pharma, Inc. During the third quarter of 2014, we discontinued applying the equity method of accounting for RXi and account for our investment in RXi as an available for sale investment.
60
LIQUIDITY AND CAPITAL RESOURCES
At December 31, 2015, we had cash and cash equivalents of approximately $193.6 million. Cash provided by operations during 2015 principally reflects the $295.0 million upfront payments received from the Pfizer Transaction, partially offset by a payment of $25.9 million to the OCS for obligations from grants previously made by the OCS to OPKO Biologics, expenses related to selling, general and administrative activities related to our corporate operations, research and development activities and our operations at Bio-Reference, OPKO Biologics, OPKO Renal and OPKO Diagnostics. We recognized $65.5 million of revenue related to the $295.0 million upfront payments received from Pfizer during the year ended December 31, 2015, and will recognize the remainder as revenue on a straight-line basis over the expected performance period. Cash used in investing activities includes the net cash used in acquisitions of $79.0 million, which reflects cash used to acquire EirGen, net and cash provided by the Bio-Reference acquisition. Cash provided by financing activities primarily reflects $25.9 million received from Common Stock option and Common Stock warrant exercises. During the year ended December 31, 2015, we also satisfied a $20.0 million contingent payment to the former owners of OPKO Renal through the issuance of 1,194,337 shares of our common stock in the third quarter of 2015. Since our inception, we have not generated gross margins sufficient to offset our operating and other expenses and our primary source of cash has been from the public and private placement of stock, the issuance of the 2033 Senior Notes and credit facilities available to us.
In January 2015, we partnered with Pfizer through a worldwide agreement for the development and commercialization of our long-acting hGH-CTP for the treatment of growth hormone deficiency (“GHD”) in adults and children, as well as for the treatment of growth failure in children born small for gestational age (“SGA”). Under the terms of the agreements with Pfizer, we received non-refundable and non-creditable upfront payments of $295.0 million in the first quarter of 2015 and are eligible to receive up to an additional $275.0 million upon the achievement of certain regulatory milestones. Pfizer received the exclusive license to commercialize hGH-CTP worldwide. In addition, we are eligible to receive initial tiered royalty payments associated with the commercialization of hGH-CTP for Adult GHD with percentage rates ranging from the high teens to mid-twenties. Upon the launch of hGH-CTP for Pediatric GHD in certain major markets, the royalties will transition to regional, tiered gross profit sharing for both hGH-CTP and Pfizer’s Genotropin®.
We will lead the clinical activities and will be responsible for funding the development programs for the key indications, which includes Adult and Pediatric GHD and Pediatric SGA. Pfizer will be responsible for all development costs for additional indications as well as all post-marketing studies. In addition, Pfizer will fund the commercialization activities for all indications and lead the manufacturing activities covered by the global development plan.
In August 2015, we completed the acquisition of Bio-Reference, the third largest full service clinical laboratory in the United States, known for its innovative technological solutions and pioneering leadership in the areas of genomics and genetic sequencing. Holders of Bio-Reference common stock received 76,566,147 shares of OPKO Common Stock for the outstanding shares of Bio-Reference common stock. The transaction was valued at approximately $950.1 million, based on a closing price per share of our Common Stock of $12.38 as reported by the New York Stock Exchange on the closing date, or $34.05 per share of Bio-Reference common stock. Included in the transaction value is $2.3 million related to the value of replacement stock option awards attributable to pre-merger service.
In May 2015, we entered into a series of purchase agreements to acquire all of the issued and outstanding shares of EirGen, a specialty pharmaceutical company incorporated in Ireland focused on the development and commercial supply of high potency, high barrier to entry pharmaceutical products, for $133.8 million in the aggregate. We acquired the outstanding shares of EirGen for approximately $100.2 million in cash and delivered 2,420,487 shares of our Common Stock valued at approximately $33.6 million based on the closing price per share of our Common Stock as reported by the New York Stock Exchange on the closing date of the acquisition, $13.88 per share.
Our licensee, TESARO, received approval by the U.S. FDA in September 2015 for oral VARUBI™, a neurokinin-1 receptor antagonist for the prevention of chemotherapy-induced nausea and vomiting. In November 2015, TESARO announced the commercial launch of VARUBI™ in the United States. We are eligible to receive milestone payments of up to $30.0 million (of which $20.0 million has been received to date) upon achievement of certain regulatory and commercial sale milestones and additional commercial milestone payments of up to $85.0 million if specified levels of annual net sales are achieved. During the years ended December 31, 2015 and 2014, $15.0 million and $5.0 million of revenue, respectively, has been recognized related to the achievement of the milestones under the TESARO License. TESARO is also obligated to pay us tiered royalties on annual net sales achieved in the United States and Europe at percentage rates that range from the low double digits to the low twenties, and outside of the United States and Europe at low double-digit percentage rates.
Under the terms of our agreement with Merck, upon approval by the FDA of the TESARO’s NDA for oral VARUBI™, which occurred in September 2015, we were required to pay Merck a $5.0 million milestone payment. In addition, $5.0 million will be due and payable each year thereafter for the next four (4) years on the anniversary date of the NDA approval. We
61
recognized the present value of the milestone payments on FDA approval of $23.0 million as an intangible asset which will be amortized to expense over the expected useful life of the asset, which is approximately 13 years. The present value of the future payments to Merck of $18.2 million at December 31, 2015 is recorded as a liability in our Consolidated Balance Sheet with $5.0 million in Accrued expenses and $13.2 million in Other long-term liabilities.
2033 Senior Notes. In January 2013, we issued $175.0 million of the 2033 Senior Notes. The 2033 Senior Notes were sold in a private placement in reliance on exemptions from registration under the Securities Act. Net cash proceeds from the offering totaled $170.2 million. Holders of the 2033 Senior Notes may require us to repurchase the 2033 Senior Notes for 100% of their principal amount, plus accrued and unpaid interest, on February 1, 2019, February 1, 2023 and February 1, 2028, or following the occurrence of a fundamental change as defined in the indenture governing the 2033 Senior Notes.
In August 2013 and June 2014, holders exchanged or converted $16.9 million and $70.4 million principal amount of 2033 Senior Notes, respectively.
On April 1, 2015, we announced that our 2033 Senior Notes were convertible through June 2015 by holders of such notes. This conversion right was triggered because the closing price per share of our Common Stock had exceeded $9.19, or 130% of the initial conversion price of $7.07, for at least 3 of 30 consecutive trading days during the period ending on March 31, 2015. Our 2033 Senior Notes continued to be convertible by holders of such notes for the remainder of 2015 and the first quarter of 2016. During 2015, pursuant to the conversion right or through exchange agreements we entered with certain holders of our 2033 Senior Notes, holders of our 2033 Senior Notes converted or exchanged $55.4 million in aggregate principal amount of 2033 Senior Notes for 8,118,062 shares of the Company’s Common Stock. At December 31, 2015, $32.2 million principal amount of 2033 Senior Notes was outstanding.
In connection with our acquisitions of CURNA, OPKO Diagnostics, OPKO Health Europe and OPKO Renal, we agreed to pay future consideration to the sellers upon the achievement of certain events, including up to an additional $19.1 million in shares of our Common Stock to the former stockholders of OPKO Diagnostics upon and subject to the achievement of certain milestones; and up to an additional $150.0 million in either shares of our Common Stock or cash, at our option subject to the achievement of certain milestones, to the former shareholders of OPKO Renal.
As of December 31, 2015, the total availability under our Credit Agreement with JPMorgan Chase Bank, N.A. (“CB”) and our lines of credit with financial institutions in Chile and Spain was $189.8 million, of which $82.7 million was used and outstanding at December 31, 2015. The weighted average interest rate on these lines of credit is approximately 4.3%. These lines of credit are short-term and are used primarily as a source of working capital. The highest balance at any time during the year ended December 31, 2015, was $91.5 million. We intend to continue to enter into these lines of credit as needed. There is no assurance that these lines of credit or other funding sources will be available to us on acceptable terms, or at all, in the future.
On November 5, 2015, Bio-Reference and certain of its subsidiaries entered into a credit agreement with CB, as lender and administrative agent (the “Credit Agreement”), which replaced Bio-Reference’s existing Credit Facility with PNC Bank, National Association (“PNC”). The Credit Agreement provides for a $175.0 million secured revolving credit facility and includes a $20.0 million sub-facility for swingline loans and a $20.0 million sub-facility for the issuance of letters of credit. Bio-Reference may increase the credit facility to up to $275.0 million on a secured basis, subject to the satisfaction of specified conditions. The Credit Agreement matures on November 5, 2020 and is guaranteed by all of Bio-Reference’s domestic subsidiaries. The Credit Agreement is also secured by substantially all assets of Bio-Reference and its domestic subsidiaries, as well as a non-recourse pledge by us of our equity interest in Bio-Reference. Availability under the Credit Agreement is based on a borrowing base comprised of eligible accounts receivables of Bio-Reference and certain of its subsidiaries, as specified therein. The proceeds of the new credit facility were used to refinance existing indebtedness, including amounts outstanding under the credit facility with PNC which was terminated in 2015 in accordance with its terms, to finance working capital needs and for general corporate purposes of Bio-Reference and its subsidiaries.
We expect to continue to incur losses from operations. We expect to incur substantial research and development expenses, including expenses related to the hiring of personnel and additional clinical trials. We expect that selling, general and administrative expenses will also increase as we expand our sales, marketing and administrative staff and add infrastructure.
We believe that the cash and cash equivalents on hand at December 31, 2015, and the amounts available to be borrowed under our lines of credit are sufficient to meet our anticipated cash requirements for operations and debt service beyond the next 12 months. We based this estimate on assumptions that may prove to be wrong or are subject to change, and we may be required to use our available cash resources sooner than we currently expect. If we acquire additional assets or companies, accelerate our product development programs or initiate additional clinical trials, we will need additional funds. Our future cash requirements will depend on a number of factors, including our relationship with Pfizer, our merger with Bio-Reference, possible acquisitions, the continued progress of research and development of our product candidates, the timing and outcome of
62
clinical trials and regulatory approvals, the costs involved in preparing, filing, prosecuting, maintaining, defending, and enforcing patent claims and other intellectual property rights, the status of competitive products, the availability of financing, and our success in developing markets for our product candidates. If we are not able to secure additional funding when needed, we may have to delay, reduce the scope of, or eliminate one or more of our clinical trials or research and development programs or possible acquisitions.
The following table provides information as of December 31, 2015, with respect to the amounts and timing of our known contractual obligation payments due by period.
|
Contractual obligations
(In thousands)
|
2016 |
2017 |
2018 |
2019 |
2020 |
Thereafter |
Total |
|||||||||||||||||||||
Open purchase orders |
$ |
48,258 |
$ |
— |
$ |
— |
$ |
— |
$ |
— |
$ |
— |
$ |
48,258 |
||||||||||||||
Operating leases |
15,830 |
10,749 |
7,862 |
6,558 |
3,208 |
7,525 |
51,732 |
|||||||||||||||||||||
Capital leases |
5,762 |
3,951 |
2,607 |
1,386 |
603 |
794 |
15,103 |
|||||||||||||||||||||
2033 Senior Notes |
— |
— |
— |
32,200 |
— |
— |
32,200 |
|||||||||||||||||||||
Deferred payments |
5,000 |
5,000 |
5,000 |
5,000 |
— |
— |
20,000 |
|||||||||||||||||||||
Mortgages and other debts payable |
2,493 |
293 |
245 |
236 |
234 |
955 |
4,456 |
|||||||||||||||||||||
Lines of credit |
83,250 |
— |
— |
— |
— |
— |
83,250 |
|||||||||||||||||||||
Interest commitments |
1,351 |
1,031 |
1,020 |
207 |
32 |
60 |
3,701 |
|||||||||||||||||||||
Total |
$ |
161,944 |
$ |
21,024 |
$ |
16,734 |
$ |
45,587 |
$ |
4,077 |
$ |
9,334 |
$ |
258,700 |
||||||||||||||
The preceding table does not include information where the amounts of the obligations are not currently determinable, including the following:
- Contractual obligations in connection with clinical trials, which span over two years, and that depend on patient enrollment. The total amount of expenditures is dependent on the actual number of patients enrolled and as such, the contracts do not specify the maximum amount we may owe.
- Product license agreements effective during the lesser of 15 years or patent expiration whereby payments and amounts are determined by applying a royalty rate on uncapped future sales.
- Contingent consideration that includes payments upon achievement of certain milestones including meeting development milestones such as the completion of successful clinical trials, NDA approvals by the FDA and revenue milestones upon the achievement of certain revenue targets all of which are anticipated to be paid within the next seven years and are payable in either shares of our Common Stock or cash, at our option, and that may aggregate up to $189.6 million.
63
CRITICAL ACCOUNTING POLICIES AND ESTIMATES
Accounting estimates. The preparation of financial statements in conformity with accounting principles generally accepted in the United States requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenues and expenses during the reporting period. Actual results could differ significantly from these estimates.
Goodwill and Intangible Assets. Goodwill represents the difference between the purchase price and the estimated fair value of the net assets acquired when accounted for by the acquisition method of accounting. Goodwill and other intangible assets, including IPR&D, acquired in business combinations, licensing and other transactions was $2.2 billion and $1.1 billion at both December 31, 2015 and 2014, respectively, representing approximately 78% and 85% of total assets, respectively.
Assets acquired and liabilities assumed in business combinations, licensing and other transactions are generally recognized at the date of acquisition at their respective fair values. Any excess of the purchase price over the estimated fair values of the net assets acquired is recognized as goodwill. We determined the fair value of intangible assets, including IPR&D, using the “income method.” This method starts with a forecast of net cash flows, risk adjusted for estimated probabilities of technical and regulatory success (for IPR&D) and adjusted to present value using an appropriate discount rate that reflects the risk associated with the cash flow streams. All assets are valued from a market participant view which might be different than our specific views. The valuation process is very complex and requires significant input and judgment using internal and external sources. Although the valuations are required to be finalized within a one-year period, it must consider all and only those facts and evidence which existed at the acquisition date. The most complex and judgmental matters applicable to the valuation process are summarized below:
• |
Unit of account – Most intangible assets are valued as single global assets rather than multiple assets for each jurisdiction or indication after considering the development stage, expected levels of incremental costs to obtain additional approvals, risks associated with further development, amount and timing of benefits expected to be derived in the future, expected patent lives in various jurisdictions and the intention to promote the asset as a global brand. |
• |
Estimated useful life – The asset life expected to contribute meaningful cash flows is determined after considering all pertinent matters associated with the asset, including expected regulatory approval dates (if unapproved), exclusivity periods and other legal, regulatory or contractual provisions as well as the effects of any obsolescence, demand, competition, and other economic factors, including barriers to entry. |
• |
Probability of Technical and Regulatory Success (“PTRS”) Rate – PTRS rates are determined based upon industry averages considering the respective programs development stage and disease indication and adjusted for specific information or data known at the acquisition date. Subsequent clinical results or other internal or external data obtained could alter the PTRS rate and materially impact the estimated fair value of the intangible asset in subsequent periods leading to impairment charges. |
• |
Projections – Future revenues are estimated after considering many factors such as initial market opportunity, pricing, sales trajectories to peak sales levels, competitive environment and product evolution. Future costs and expenses are estimated after considering historical market trends, market participant synergies and the timing and level of additional development costs to obtain the initial or additional regulatory approvals, maintain or further enhance the product. We generally assume initial positive cash flows to commence shortly after the receipt of expected regulatory approvals which typically may not occur for a number of years. Actual cash flows attributed to the project are likely to be different than those assumed since projections are subjected to multiple factors including trial results and regulatory matters which could materially change the ultimate commercial success of the asset as well as significantly alter the costs to develop the respective asset into commercially viable products. |
• |
Tax rates – The expected future income is tax effected using a market participant tax rate. Our recent valuations typically use a U.S. tax rate (and applicable state taxes) after considering the jurisdiction in which the intellectual property is held and location of research and manufacturing infrastructure. We also considered that any repatriation of earnings would likely have U.S. tax consequences. |
• |
Discount rate – Discount rates are selected after considering the risks inherent in the future cash flows; the assessment of the asset’s life cycle and the competitive trends impacting the asset, including consideration of any technical, legal, regulatory, or economic barriers to entry, as well as expected changes in standards of practice for indications addressed by the asset. |
Goodwill was $743.3 million and $224.3 million, respectively, at December 31, 2015 and 2014. The increase in goodwill from December 31, 2014 to 2015 is due to goodwill recognized from the acquisitions of Bio-Reference and EirGen in August 2015 and May 2015, respectively. Goodwill is tested at least annually for impairment or when events or changes in
64
circumstances indicate that the carrying amount of such assets may not be recoverable, on an enterprise level by assessing qualitative factors or performing a quantitative analysis in determining whether it is more likely than not that its fair value exceeds the carrying value. Examples of qualitative factors include our share price, our financial performance compared to budgets, long-term financial plans, macroeconomic, industry and market conditions as well as the substantial excess of fair value over the carrying value of net assets from the annual impairment test previously performed. We recorded $87,000 of goodwill impairment during the year ended December 31, 2015 as a result of our testing. No goodwill impairment was recorded for the year ended December 31, 2014 as a result of our testing.
The estimated fair value of a reporting unit is highly sensitive to changes in projections and assumptions; therefore, in some instances changes in these assumptions could potentially lead to impairment. We perform sensitivity analyses around our assumptions in order to assess the reasonableness of the assumptions and the results of our testing. Ultimately, future potential changes in these assumptions may impact the estimated fair value of a reporting unit and cause the fair value of the reporting unit to be below its carrying value. We believe that our estimates are consistent with assumptions that marketplace participants would use in their estimates of fair value. However, if actual results are not consistent with our estimates and assumptions, we may be exposed to an impairment charge that could be material.
Intangible assets were $1.4 billion and $855.8 million, including IPR&D of $792.3 million and $793.2 million, respectively, at December 31, 2015 and 2014. The increase in intangible assets from December 31, 2014 to 2015 is due to intangible assets recognized from the acquisitions of Bio-Reference and EirGen in August 2015 and May 2015, respectively. Intangible assets are tested for impairment whenever events or changes in circumstances indicate that the carrying amount of such assets may not be recoverable, although IPR&D is required to be tested at least annually until the project is completed or abandoned. Upon obtaining regulatory approval, the IPR&D asset is then accounted for as a finite-lived intangible asset and amortized on a straight-line basis over its estimated useful life. If the project is abandoned, the IPR&D asset is charged to expense.
Intangible assets are highly vulnerable to impairment charges, particularly newly acquired assets for recently launched products or IPR&D. These assets are initially measured at fair value and therefore any reduction in expectations used in the valuations could potentially lead to impairment. Some of the more common potential risks leading to impairment include competition, earlier than expected loss of exclusivity, pricing pressures, adverse regulatory changes or clinical trial results, delay or failure to obtain regulatory approval and additional development costs, inability to achieve expected synergies, higher operating costs, changes in tax laws and other macro-economic changes. The complexity in estimating the fair value of intangible assets in connection with an impairment test is similar to the initial valuation.
Considering the high risk nature of research and development and the industry’s success rate of bringing developmental compounds to market, IPR&D impairment charges are likely to occur in future periods. IPR&D is closely monitored and assessed each period for impairment.
We amortize intangible assets with definite lives on a straight-line basis over their estimated useful lives, currently ranging from 3 to 20 years. We use the straight-line method of amortization as there is no reliably determinable pattern in which the economic benefits of our intangible assets are consumed or otherwise used up. Amortization expense was $28.0 million and $10.9 million for the years ended December 31, 2015 and 2014, respectively.
Revenue recognition. Revenue for laboratory services is recognized at the time test results are reported, which approximates when services are provided. Services are provided to patients covered by various third-party payer programs including various managed care organizations, as well as the Medicare and Medicaid programs. Billings for services under third-party payer programs are included in revenue net of allowances for contractual discounts and allowances for differences between the amounts billed and estimated program payment amounts. Adjustments to the estimated payment amounts based on final settlement with the programs are recorded upon settlement as an adjustment to revenue. For the years ended December 31, 2015 and 2014, approximately 9% and 5%, respectively, of our revenues were derived directly from the Medicare and Medicaid programs. The increase in revenues from laboratory services, including revenue from Medicare and Medicaid programs, is due to the acquisition of Bio-Reference in August 2015.
Generally, we recognize revenue from product sales when goods are shipped and title and risk of loss transfer to our customers. Our estimates for sales returns and allowances are based upon the historical patterns of product returns and allowances taken, matched against the sales from which they originated, and management’s evaluation of specific factors that may increase or decrease the risk of product returns.
Revenue from transfer of intellectual property includes revenue related to the sale, license or transfer of intellectual property such as upfront license payments, license fees and milestone payments received through our license, collaboration and commercialization agreements. We analyze our multiple-element arrangements to determine whether the elements can be separated and accounted for individually as separate units of accounting.
65
Non-refundable license fees for the out-license of our technology are recognized depending on the provisions of each agreement. We recognize non-refundable upfront license payments as revenue upon receipt if the license has standalone value and qualifies for treatment as a separate unit of accounting under multiple-element arrangement guidance. License fees with ongoing involvement or performance obligations that do not have standalone value are recorded as deferred revenue, included in Accrued expenses or Other long-term liabilities, when received and generally are recognized ratably over the period of such performance obligations only after both the license period has commenced and we have delivered the technology.
The assessment of our obligations and related performance periods requires significant management judgment. If an agreement contains research and development obligations, the relevant time period for the research and development phase is based on management estimates and could vary depending on the outcome of clinical trials and the regulatory approval process. Such changes could materially impact the revenue recognized, and as a result, management reviews the estimates related to the relevant time period of research and development on a quarterly basis.
Revenue from milestone payments related to arrangements under which we have continuing performance obligations is recognized as Revenue from transfer of intellectual property upon achievement of the milestone only if all of the following conditions are met: the milestone payments are non-refundable; there was substantive uncertainty at the date of entering into the arrangement that the milestone would be achieved; the milestone is commensurate with either our performance to achieve the milestone or the enhancement of the value of the delivered item by us; the milestone relates solely to past performance; and the amount of the milestone is reasonable in relation to the effort expended or the risk associated with the achievement of the milestone. If any of these conditions are not met, the milestone payments are not considered to be substantive and are, therefore, deferred and recognized as Revenue from transfer of intellectual property over the term of the arrangement as we complete our performance obligations.
Concentration of Credit Risk and Allowance for doubtful accounts. Financial instruments that potentially subject us to concentrations of credit risk consist primarily of accounts receivable. Substantially all of our accounts receivable are with companies in the health care industry and individuals. However, concentrations of credit risk are limited due to the number of our clients as well as their dispersion across many different geographic regions.
While we have receivables due from federal and state governmental agencies, we do not believe that such receivables represent a credit risk since the related health care programs are funded by federal and state governments, and payment is primarily dependent upon submitting appropriate documentation. Accounts receivable balances (prior to allowance for doubtful accounts and net of contractual adjustments) from Medicare and Medicaid were $26.1 million and $0.6 million at December 31, 2015 and 2014, respectively.
The portion of our accounts receivable due from patients comprises the largest portion of credit risk. At December 31, 2015 and 2014, receivables due from patients represent approximately 7.5% and 0.5% of our consolidated accounts receivable (prior to allowance for doubtful accounts and net of contractual adjustments).
We assess the collectability of accounts receivable balances by considering factors such as historical collection experience, customer credit worthiness, the age of accounts receivable balances, regulatory changes and current economic conditions and trends that may affect a customer’s ability to pay. Actual results could differ from those estimates. Our reported net income (loss) is directly affected by our estimate of the collectability of accounts receivable. The allowance for doubtful accounts recognized in our Consolidated Balance Sheets was $25.2 million and $1.9 million at December 31, 2015 and 2014, respectively.
Income Taxes. Income taxes are accounted for under the asset-and-liability method. Deferred tax assets and liabilities are recognized for the future tax consequences attributable to differences between the financial statement carrying amounts of existing assets and liabilities and the respective tax bases and operating loss and tax credit carryforwards. Deferred tax assets and liabilities are measured using enacted tax rates expected to apply to taxable income in the years in which those temporary differences are expected to be recovered or settled. The effect on deferred tax assets and liabilities of a change in tax rates is recognized in operations in the period that includes the enactment date. We periodically evaluate the realizability of our net deferred tax assets. Our tax accruals are analyzed periodically and adjustments are made as events occur to warrant such adjustment.
Equity-based compensation. We measure the cost of employee services received in exchange for an award of equity instruments based on the grant-date fair value of the award. That cost is recognized in the Consolidated Statement of Operations over the period during which an employee is required to provide service in exchange for the award. We record excess tax benefits, realized from the exercise of stock options as a financing cash inflow and as a reduction of taxes paid in cash flow from operations. Equity-based compensation arrangements to non-employees are recorded at their fair value on the measurement date. The measurement of equity-based compensation to non-employees is subject to periodic adjustment as the underlying equity instruments vest. We estimate the grant-date fair value of our stock option grants using a valuation model
66
known as the Black-Scholes-Merton formula or the “Black-Scholes Model.” The Black-Scholes Model requires the use of several variables to estimate the grant-date fair value of stock options including expected term, expected volatility, expected dividends and risk-free interest rate. We perform analyses to calculate and select the appropriate variable assumptions used in the Black-Scholes Model and to estimate forfeitures of equity-based awards. We are required to adjust our forfeiture estimates on at least an annual basis based on the number of share-based awards that ultimately vest. The selection of assumptions and estimated forfeiture rates is subject to significant judgment and future changes to our assumptions and estimates which may have a material impact on our Consolidated Financial Statements.
Inventories. Inventories are valued at the lower of cost or market (net realizable value). Cost is determined by the first-in, first-out method. We consider such factors as the amount of inventory on hand, estimated time required to sell such inventories, remaining shelf-life, and current market conditions to determine whether inventories are stated at the lower of cost or market. Inventories at our diagnostics segment consist primarily of purchased laboratory supplies, which is used in our testing laboratories.
Pre-launch inventories. We may accumulate commercial quantities of certain product candidates prior to the date we anticipate that such products will receive final U.S. FDA approval. The accumulation of such pre-launch inventories involves the risk that such products may not be approved for marketing by the FDA on a timely basis, or ever. This risk notwithstanding, we may accumulate pre-launch inventories of certain products when such action is appropriate in relation to the commercial value of the product launch opportunity. In accordance with our policy, this pre-launch inventory is expensed.
Contingent consideration. Each period we revalue the contingent consideration obligations associated with certain acquisitions to their fair value and record increases in the fair value as contingent consideration expense and decreases in the fair value as contingent consideration income. Changes in contingent consideration result from changes in the assumptions regarding probabilities of successful achievement of related milestones, the estimated timing in which the milestones are achieved and the discount rate used to estimate the fair value of the liability. Contingent consideration may change significantly as our development programs progress, revenue estimates evolve and additional data is obtained, impacting our assumptions. The assumptions used in estimating fair value require significant judgment. The use of different assumptions and judgments could result in a materially different estimate of fair value which may have a material impact on our results from operations and financial position.
67
RECENT ACCOUNTING PRONOUNCEMENTS
In May 2014, the FASB issued Accounting Standards Update (“ASU”), ASU No. 2014-09, “Revenue from Contracts with Customers.” ASU No. 2014-09 clarifies the principles for recognizing revenue and develops a common revenue standard for GAAP and International Financial Reporting Standards that removes inconsistencies and weaknesses in revenue requirements, provides a more robust framework for addressing revenue issues, improves comparability of revenue recognition practices across entities, industries, jurisdictions, and capital markets, provides more useful information to users of financial statements through improved disclosure requirements and simplifies the preparation of financial statements by reducing the number of requirements to which an entity must refer. ASU No. 2014-09 is effective for fiscal years, and interim periods within those years, beginning after December 15, 2017. Companies can choose to apply the ASU using either the full retrospective approach or a modified retrospective approach. We are currently evaluating both methods of adoption and the impact that the adoption of this ASU will have on our Consolidated Financial Statements.
In June 2014, the FASB issued ASU No. 2014-12, “Accounting for Share-Based Payments When the Terms of an Award Provide That a Performance Target Could Be Achieved after the Requisite Service Period (a consensus of the FASB Emerging Issues Task Force).” ASU No. 2014-12 requires that a performance target that affects vesting and that could be achieved after the requisite service period be treated as a performance condition. ASU No. 2014-12 is effective for fiscal years, and interim periods within those years, beginning after December 15, 2015. Earlier adoption is permitted. The amendments can be applied either prospectively to all awards granted or modified after the effective date or retrospectively to all awards with performance targets that are outstanding as of the beginning of the earliest annual period presented in the financial statements and to all new or modified awards. We expect to apply the ASU prospectively and do not expect the adoption to have an impact on our Consolidated Financial Statements.
In August 2014, the FASB issued ASU No. 2014-15, “Disclosure of Uncertainties about an Entity’s Ability to Continue as a Going Concern,” to provide guidance on management’s responsibility in evaluating whether there is substantial doubt about a company’s ability to continue as a going concern and to provide related footnote disclosures. ASU 2014-15 is effective for annual periods ending after December 15, 2016 with early adoption permitted. We do not believe the impact of our pending adoption of ASU 2014-15 on our Consolidated Financial Statements will be material.
In February 2015, the FASB issued ASU No. 2015-02, “Consolidation (Topic 810): Amendments to the Consolidation Analysis,” which amends current consolidation guidance including changes to both the variable and voting interest models used by companies to evaluate whether an entity should be consolidated. The requirements from ASU 2015-02 are effective for interim and annual periods beginning after December 15, 2015, with early adoption permitted. We do not believe the impact of our pending adoption of ASU 2015-02 on our Consolidated Financial Statements will be material.
In July 2015, the FASB issued ASU No. 2015-11, “Inventory (Topic 330): Simplifying the Measurement of Inventory,” which changes the measurement principle for entities that do not measure inventory using the last-in, first-out (“LIFO”) or retail inventory method from the lower of cost or market to lower of cost and net realizable value. ASU 2015-11 is effective for fiscal years beginning after December 15, 2016, including interim periods within those fiscal years, with early adoption permitted. We are currently evaluating the impact of this new guidance on our Consolidated Financial Statements.
In September 2015, the FASB issued ASU No. 2015-16, “Business Combinations (Topic 805): Simplifying the Accounting for Measurement-Period Adjustments,” which replaces the requirement that an acquirer in a business combination account for measurement period adjustments retrospectively with a requirement that an acquirer recognize adjustments to the provisional amounts that are identified during the measurement period in the reporting period in which the adjustment amounts are determined. ASU 2015-16 requires that the acquirer record, in the same period’s financial statements, the effect on earnings of changes in depreciation, amortization, or other income effects, if any, as a result of the change to the provisional amounts, calculated as if the accounting had been completed at the acquisition date. ASU 2015-16 is effective for fiscal years beginning after December 15, 2015, including interim periods within those fiscal years. The guidance is to be applied prospectively to adjustments to provisional amounts that occur after the effective date of the guidance, with earlier application permitted for financial statements that have not been issued. Our early adoption of ASU 2015-16 in the third quarter of 2015 did not have a material impact on our Consolidated Financial Statements.
In November 2015, the FASB issued ASU No. 2015-17, “Income Taxes (Topic 740): Balance Sheet Classification of Deferred Taxes,” which requires deferred tax liabilities and assets to be classified as noncurrent in a classified statement of financial position. ASU 2015-17 is effective for financial statements issued for annual periods beginning after December 15, 2016, and interim periods within those annual periods. Earlier application is permitted for all entities as of the beginning of an interim or annual reporting period. We adopted the provisions of this ASU prospectively in the fourth quarter of 2015, and did not retrospectively adjust the prior periods. The adoption of this ASU will simplify the presentation of deferred income taxes and reduce complexity without decreasing the usefulness of information provided to users of financial statements. The
68
adoption of ASU 2015-17 did not have a significant impact on our financial position, results of operations and cash flows.
69
ITEM 7A. QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK
In the normal course of doing business, we are exposed to the risks associated with foreign currency exchange rates and changes in interest rates.
Foreign Currency Exchange Rate Risk – We operate globally and, as such, we are subject to foreign exchange risk in our commercial operations as a significant portion of our revenues are exposed to changes in foreign currency exchange rates, primarily the Chilean peso, the Mexican peso, the Euro and the New Israeli shekel.
Although we do not speculate in the foreign exchange market, we may from time to time manage exposures that arise in the normal course of business related to fluctuations in foreign currency exchange rates by entering into offsetting positions through the use of foreign exchange forward contracts. Certain firmly committed transactions may be hedged with foreign exchange forward contracts. As exchange rates change, gains and losses on the exposed transactions are partially offset by gains and losses related to the hedging contracts. Both the exposed transactions and the hedging contracts are translated and fair valued, respectively, at current spot rates, with gains and losses included in earnings.
Our derivative activities, which consist of foreign exchange forward contracts, are initiated to hedge forecasted cash flows that are exposed to foreign currency risk. The foreign exchange forward contracts generally require us to exchange local currencies for foreign currencies based on pre-established exchange rates at the contracts’ maturity dates. As exchange rates change, gains and losses on these contracts are generated based on the change in the exchange rates that are recognized in the Consolidated Statement of Operations and offset the impact of the change in exchange rates on the foreign currency cash flows that are hedged. If the counterparties to the exchange contracts do not fulfill their obligations to deliver the contracted currencies, we could be at risk for currency related fluctuations. We had $6.2 million in foreign exchange forward contracts outstanding at December 31, 2015, primarily to hedge Chilean-based operating cash flows against U.S. dollars. If Chilean pesos were to strengthen or weaken in relation to the U.S. dollar, our loss or gain on hedged foreign currency cash-flows would be offset by the derivative contracts, with a net effect of zero.
We do not engage in trading market risk sensitive instruments or purchasing hedging instruments or “other than trading” instruments that are likely to expose us to significant market risk, whether interest rate, foreign currency exchange, commodity price, or equity price risk.
Interest Rate Risk – Our exposure to interest rate risk relates to our cash and investments and to our borrowings. We maintain an investment portfolio of money market funds. The securities in our investment portfolio are not leveraged, and are, due to their very short-term nature, subject to minimal interest rate risk. We currently do not hedge interest rate exposure. Because of the short-term maturities of our investments, we do not believe that a change in market interest rates would have a significant negative impact on the value of our investment portfolio except for reduced income in a low interest rate environment.
At December 31, 2015, we had cash and cash equivalents and marketable securities of $193.6 million. The weighted average interest rate related to our cash and cash equivalents for the years ended December 31, 2015 was 0%. As of December 31, 2015, the principal outstanding balance under our Credit Agreement with JPMorgan Chase Bank, N.A. and our Chilean and Spanish credit lines was $82.7 million in the aggregate at a weighted average interest rate of approximately 4.3%.
Our $32.2 million aggregate principal amount of our 2033 Senior Notes has a fixed interest rate, and therefore is not subject to fluctuations in market interest rates.
The primary objective of our investment activities is to preserve principal while at the same time maximizing yields without significantly increasing risk. To achieve this objective, we invest our excess cash in debt instruments of the U.S. Government and its agencies, bank obligations, repurchase agreements and high-quality corporate issuers, and money market funds that invest in such debt instruments, and, by policy, restrict our exposure to any single corporate issuer by imposing concentration limits. To minimize the exposure due to adverse shifts in interest rates, we maintain investments at an average maturity of generally less than three months.
Equity Price Risk – We are subject to equity price risk related to the (i) rights to convert into shares of our Common Stock, including upon a fundamental change; and (ii) a coupon make-whole payment in the event of a conversion by the holders of the 2033 Senior Notes on or after February 1, 2017 but prior to February 1, 2019. These terms are considered to be embedded derivatives. On a quarterly basis, we are required to record these embedded derivatives at fair value with the changes being recorded in our Consolidated Statement of Operations. Accordingly, our results of operations are subject to exposure associated with increases or decreases in the estimated fair value of our embedded derivatives.
70
ITEM 8. FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA
Page |
|
71
Report of Independent Registered Certified Public Accounting Firm
The Board of Directors and Shareholders of OPKO Health, Inc. and subsidiaries
We have audited the accompanying consolidated balance sheets of OPKO Health, Inc. and subsidiaries as of December 31, 2015 and 2014, and the related consolidated statements of operations, comprehensive loss, equity and cash flows for each of the three years in the period ended December 31, 2015. These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements. An audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the financial statements referred to above present fairly, in all material respects, the consolidated financial position of OPKO Health, Inc. and subsidiaries at December 31, 2015 and 2014, and the consolidated results of their operations and their cash flows for each of the three years in the period ended December 31, 2015, in conformity with U.S. generally accepted accounting principles.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), OPKO Health, Inc. and subsidiaries’ internal control over financial reporting as of December 31, 2015, based on criteria established in Internal Control-Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (2013 framework) and our report dated February 29, 2016 expressed an unqualified opinion thereon.
/s/ Ernst & Young LLP
Miami, Florida
February 29, 2016
72
Report of Independent Registered Certified Public Accounting Firm
The Board of Directors and Shareholders of OPKO Health, Inc. and subsidiaries
We have audited OPKO Health, Inc. and subsidiaries’ internal control over financial reporting as of December 31, 2015, based on criteria established in Internal Control-Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (2013 framework) (the “COSO criteria”). OPKO Health, Inc. and subsidiaries’ management is responsible for maintaining effective internal control over financial reporting, and for its assessment of the effectiveness of internal control over financial reporting included in the accompanying Management’s Annual Report on Internal Control Over Financial Reporting. Our responsibility is to express an opinion on the Company’s internal control over financial reporting based on our audit.
We conducted our audit in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects. Our audit included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, testing and evaluating the design and operating effectiveness of internal control based on the assessed risk, and performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
As indicated in the accompanying Management’s Annual Report on Internal Control Over Financial Reporting, management’s assessment of and conclusion on the effectiveness of internal control over financial reporting did not include the internal controls of Bio-Reference Laboratories, Inc. and EirGen Pharma Limited, which are included in the December 31, 2015 consolidated financial statements of OPKO Health, Inc. and subsidiaries and constituted 15% of consolidated total assets, as of December 31, 2015 and 68% of consolidated revenues, for the year then ended. Our audit of internal control over financial reporting of OPKO Health, Inc. and subsidiaries also did not include an evaluation of the internal control over financial reporting of Bio-Reference Laboratories, Inc. or EirGen Pharma Limited.
In our opinion, OPKO Health, Inc. and subsidiaries maintained, in all material respects, effective internal control over financial reporting as of December 31, 2015, based on the COSO criteria.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), the consolidated balance sheets of OPKO Health, Inc. and subsidiaries as of December 31, 2015 and 2014, and the related consolidated statements of operations, comprehensive loss, equity and cash flows for each of the three years in the period ended December 31, 2015 of OPKO Health, Inc. and subsidiaries and our report dated February 29, 2016 expressed an unqualified opinion thereon.
/s/ Ernst & Young LLP
Miami, Florida
February 29, 2016
73
OPKO Health, Inc. and Subsidiaries
CONSOLIDATED BALANCE SHEETS
(In thousands, except share and per share data)
December 31, |
|||||||
2015 |
2014(1)
|
||||||
ASSETS |
|||||||
Current assets: |
|||||||
Cash and cash equivalents |
$ |
193,598 |
$ |
96,907 |
|||
Accounts receivable, net |
193,875 |
19,969 |
|||||
Inventory, net |
39,681 |
16,604 |
|||||
Prepaid expenses and other current assets |
26,904 |
9,389 |
|||||
Total current assets |
454,058 |
142,869 |
|||||
Property, plant and equipment, net |
131,798 |
16,411 |
|||||
Intangible assets, net |
638,152 |
62,649 |
|||||
In-process research and development |
792,275 |
793,152 |
|||||
Goodwill |
743,348 |
224,292 |
|||||
Investments, net |
34,716 |
22,453 |
|||||
Other assets |
5,267 |
5,838 |
|||||
Total assets |
$ |
2,799,614 |
$ |
1,267,664 |
|||
LIABILITIES AND EQUITY |
|||||||
Current liabilities: |
|||||||
Accounts payable |
$ |
72,535 |
$ |
8,744 |
|||
Accrued expenses |
167,899 |
60,912 |
|||||
Current portion of lines of credit and notes payable |
11,468 |
13,455 |
|||||
Total current liabilities |
251,902 |
83,111 |
|||||
2033 Senior Notes, net of discount and estimated fair value of embedded derivatives |
49,412 |
131,454 |
|||||
Deferred tax liabilities, net |
226,036 |
167,153 |
|||||
Other long-term liabilities, principally deferred revenue |
292,470 |
50,205 |
|||||
Total long-term liabilities |
567,918 |
348,812 |
|||||
Total liabilities |
819,820 |
431,923 |
|||||
Equity: |
|||||||
Common Stock - $0.01 par value, 750,000,000 shares authorized; 546,188,516 and 433,421,677 shares issued at December 31, 2015 and 2014, respectively |
5,462 |
4,334 |
|||||
Treasury Stock, at cost - 1,120,367 and 1,245,367 shares at December 31, 2015 and 2014, respectively |
(3,645 |
) |
(4,051 |
) |
|||
Additional paid-in capital |
2,705,385 |
1,529,096 |
|||||
Accumulated other comprehensive loss |
(22,537 |
) |
(12,392 |
) |
|||
Accumulated deficit |
(704,871 |
) |
(674,843 |
) |
|||
Total shareholders’ equity attributable to OPKO |
1,979,794 |
842,144 |
|||||
Noncontrolling interests |
— |
(6,403 |
) |
||||
Total shareholders’ equity |
1,979,794 |
835,741 |
|||||
Total liabilities and equity |
$ |
2,799,614 |
$ |
1,267,664 |
|||
(1) |
As of December 31, 2014, total assets include $7.6 million and total liabilities include $12.1 million related to SciVac Ltd (“SciVac”). SciVac was a consolidated variable interest entity which we deconsolidated in July 2015. Refer to Note 4. SciVac’s consolidated assets were owned by SciVac and SciVac’s consolidated liabilities had no recourse against us.
|
The accompanying Notes to Consolidated Financial Statements are an integral part of these statements.
74
OPKO Health, Inc. and Subsidiaries
CONSOLIDATED STATEMENTS OF OPERATIONS
(In thousands, except share and per share data)
For the years ended December 31, |
|||||||||||
2015 |
2014 |
2013 |
|||||||||
Revenues: |
|||||||||||
Revenue from services |
$ |
329,739 |
$ |
8,666 |
$ |
11,658 |
|||||
Revenue from products |
80,146 |
76,983 |
68,161 |
||||||||
Revenue from transfer of intellectual property and other |
81,853 |
5,476 |
16,711 |
||||||||
Total revenues |
491,738 |
91,125 |
96,530 |
||||||||
Costs and expenses: |
|||||||||||
Costs of service revenue |
193,305 |
9,372 |
10,419 |
||||||||
Cost of product revenue |
41,934 |
38,637 |
38,441 |
||||||||
Selling, general and administrative |
196,576 |
57,940 |
55,320 |
||||||||
Research and development |
99,488 |
83,571 |
53,902 |
||||||||
In-process research and development |
— |
12,055 |
— |
||||||||
Contingent consideration |
5,050 |
24,446 |
6,947 |
||||||||
Amortization of intangible assets |
27,977 |
10,919 |
11,133 |
||||||||
Grant repayment |
25,889 |
— |
— |
||||||||
Total costs and expenses |
590,219 |
236,940 |
176,162 |
||||||||
Operating loss |
(98,481 |
) |
(145,815 |
) |
(79,632 |
) |
|||||
Other income and (expense), net: |
|||||||||||
Interest income |
255 |
771 |
376 |
||||||||
Interest expense |
(8,419 |
) |
(12,263 |
) |
(13,802 |
) |
|||||
Fair value changes of derivative instruments, net |
(39,083 |
) |
(10,632 |
) |
(45,942 |
) |
|||||
Other income (expense), net |
7,730 |
(3,088 |
) |
34,782 |
|||||||
Other income and (expense), net |
(39,517 |
) |
(25,212 |
) |
(24,586 |
) |
|||||
Loss before income taxes and investment losses |
(137,998 |
) |
(171,027 |
) |
(104,218 |
) |
|||||
Income tax benefit (provision) |
113,675 |
(24 |
) |
(1,672 |
) |
||||||
Loss before investment losses |
(24,323 |
) |
(171,051 |
) |
(105,890 |
) |
|||||
Loss from investments in investees |
(7,105 |
) |
(3,587 |
) |
(11,456 |
) |
|||||
Net loss |
(31,428 |
) |
(174,638 |
) |
(117,346 |
) |
|||||
Less: Net loss attributable to noncontrolling interests |
(1,400 |
) |
(2,972 |
) |
(2,939 |
) |
|||||
|
Net loss attributable to common shareholders before
preferred stock dividend
|
(30,028 |
) |
(171,666 |
) |
(114,407 |
) |
|||||
Preferred stock dividend |
— |
— |
(420 |
) |
|||||||
Net loss attributable to common shareholders |
$ |
(30,028 |
) |
$ |
(171,666 |
) |
$ |
(114,827 |
) |
||
Loss per share, basic and diluted: |
|||||||||||
Net loss per share |
$ |
(0.06 |
) |
$ |
(0.41 |
) |
$ |
(0.32 |
) |
||
|
Weighted average number of common shares
outstanding, basic and diluted
|
488,065,908 |
422,014,039 |
355,095,701 |
||||||||
The accompanying Notes to Consolidated Financial Statements are an integral part of these statements.
75
OPKO Health, Inc. and Subsidiaries
CONSOLIDATED STATEMENTS OF COMPREHENSIVE LOSS
(In thousands)
For the years ended December 31, |
|||||||||||
2015 |
2014 |
2013 |
|||||||||
Net loss |
$ |
(31,428 |
) |
$ |
(174,638 |
) |
$ |
(117,346 |
) |
||
Other comprehensive income (loss), net of tax: |
|||||||||||
Change in foreign currency translation and other comprehensive income (loss) from equity investments |
(15,074 |
) |
(8,088 |
) |
(1,825 |
) |
|||||
Available for sale investments: |
|||||||||||
Change in unrealized gain (loss), net of tax |
(2,378 |
) |
(8,044 |
) |
2,467 |
||||||
Less: reclassification adjustments for (gains) losses included in net loss, net of tax |
7,307 |
322 |
(4,580 |
) |
|||||||
Comprehensive loss |
(41,573 |
) |
(190,448 |
) |
(121,284 |
) |
|||||
Less: Comprehensive loss attributable to noncontrolling interest |
(1,400 |
) |
(2,972 |
) |
(2,939 |
) |
|||||
Comprehensive loss attributable to common shareholders before preferred stock dividend |
(40,173 |
) |
(187,476 |
) |
(118,345 |
) |
|||||
Preferred stock dividend |
— |
— |
(420 |
) |
|||||||
Comprehensive loss attributable to common shareholders |
$ |
(40,173 |
) |
$ |
(187,476 |
) |
$ |
(118,765 |
) |
||
The accompanying Notes to Consolidated Financial Statements are an integral part of these statements.
76
OPKO Health, Inc. and Subsidiaries
CONSOLIDATED STATEMENTS OF EQUITY
(In thousands, except share and per share data)
For the years ended December 31, 2015, 2014, 2013 (continued)
Common Stock |
Treasury |
Additional
Paid-In
Capital
|
Accumulated Other
Comprehensive
Income
|
Accumulated
Deficit
|
Noncontrolling
Interests
|
Total |
|||||||||||||||||||||||||||
Shares |
Dollars |
Shares |
Dollars |
||||||||||||||||||||||||||||||
Balance at December 31, 2012 |
305,560,763 |
$ |
3,056 |
(2,293,056 |
) |
$ |
(7,457 |
) |
$ |
565,201 |
$ |
7,356 |
$ |
(388,770 |
) |
$ |
(492 |
) |
$ |
178,894 |
|||||||||||||
Equity-based compensation expense |
— |
— |
— |
— |
10,983 |
— |
— |
— |
10,983 |
||||||||||||||||||||||||
Exercise of Common Stock options and warrants |
10,732,745 |
107 |
— |
— |
23,317 |
— |
— |
— |
23,424 |
||||||||||||||||||||||||
Series D Preferred Stock dividend |
— |
— |
— |
— |
(3,015 |
) |
— |
— |
— |
(3,015 |
) |
||||||||||||||||||||||
|
Conversion of Series D Preferred
Stock
|
11,290,320 |
113 |
— |
— |
24,273 |
— |
— |
— |
24,386 |
||||||||||||||||||||||||
Conversion of 2033 Senior Notes |
2,396,145 |
24 |
— |
— |
20,815 |
— |
— |
— |
20,839 |
||||||||||||||||||||||||
|
Issuance of Common Stock in
connection with OPKO Brazil
acquisition at $6.73 per share
|
64,684 |
1 |
— |
— |
434 |
— |
— |
— |
435 |
||||||||||||||||||||||||
|
Issuance of Common Stock in
connection with OPKO Renal
acquisition at $7.16 per share
|
20,517,030 |
205 |
— |
— |
146,697 |
— |
— |
— |
146,902 |
||||||||||||||||||||||||
|
Issuance of Common Stock in
connection with OPKO Biologics
acquisition at $8.49 per
share and fair value of stock
options and warrants exchanged
|
63,670,805 |
637 |
— |
— |
586,006 |
— |
— |
— |
586,643 |
||||||||||||||||||||||||
|
Issuance of Common Stock in
connection with OPKO Health
Europe’s first Deferred Payment
at $7.52 per share
|
585,703 |
5 |
— |
— |
4,430 |
— |
— |
— |
4,435 |
||||||||||||||||||||||||
|
Issuance of Treasury Stock in
connection with OPKO Health
Europe’s Contingent
Consideration at $11.60 per share
|
28,993 |
95 |
242 |
337 |
|||||||||||||||||||||||||||||
|
Net loss attributable to common
shareholders before preferred
stock dividend
|
— |
— |
— |
— |
— |
— |
(114,407 |
) |
— |
(114,407 |
) |
||||||||||||||||||||||
|
Net loss attributable to
noncontrolling interests
|
— |
— |
— |
— |
— |
— |
— |
(2,939 |
) |
(2,939 |
) |
||||||||||||||||||||||
Other comprehensive loss |
— |
— |
— |
— |
(3,938 |
) |
— |
— |
(3,938 |
) |
|||||||||||||||||||||||
Balance at December 31, 2013 |
414,818,195 |
$ |
4,148 |
(2,264,063 |
) |
$ |
(7,362 |
) |
$ |
1,379,383 |
$ |
3,418 |
$ |
(503,177 |
) |
$ |
(3,431 |
) |
$ |
872,979 |
|||||||||||||
The accompanying Notes to Consolidated Financial Statements are an integral part of these statements.
77
OPKO Health, Inc. and Subsidiaries
CONSOLIDATED STATEMENTS OF EQUITY
(In thousands, except share and per share data)
For the years ended December 31, 2015, 2014, 2013 (continued)
Common Stock |
Treasury |
Additional
Paid-In
Capital
|
Accumulated Other
Comprehensive
Income (Loss)
|
Accumulated
Deficit
|
Noncontrolling
Interests
|
Total |
|||||||||||||||||||||||||||
Shares |
Dollars |
Shares |
Dollars |
||||||||||||||||||||||||||||||
Balance at December 31, 2013 |
414,818,195 |
$ |
4,148 |
(2,264,063 |
) |
$ |
(7,362 |
) |
$ |
1,379,383 |
$ |
3,418 |
$ |
(503,177 |
) |
$ |
(3,431 |
) |
$ |
872,979 |
|||||||||||||
Equity-based compensation expense |
— |
— |
— |
— |
14,737 |
— |
— |
— |
14,737 |
||||||||||||||||||||||||
Exercise of Common Stock options and warrants |
5,392,841 |
54 |
— |
— |
12,874 |
— |
— |
— |
12,928 |
||||||||||||||||||||||||
Issuance of Common Stock for OPKO Uruguay |
— |
— |
19,140 |
61 |
98 |
— |
— |
— |
159 |
||||||||||||||||||||||||
Issuance of Common Stock upon exchange of 2033 Senior Notes |
10,974,431 |
110 |
— |
— |
95,555 |
— |
— |
— |
95,665 |
||||||||||||||||||||||||
Issuance of Common Stock for Inspiro at $8.57 |
— |
— |
999,556 |
3,250 |
5,316 |
— |
— |
— |
8,566 |
||||||||||||||||||||||||
Issuance of Common Stock for OPKO Renal earnout |
2,236,210 |
22 |
— |
— |
21,133 |
— |
— |
— |
21,155 |
||||||||||||||||||||||||
Net loss attributable to common shareholders |
— |
— |
— |
— |
— |
— |
(171,666 |
) |
— |
(171,666 |
) |
||||||||||||||||||||||
Net loss attributable to noncontrolling interests |
— |
— |
— |
— |
— |
— |
— |
(2,972 |
) |
(2,972 |
) |
||||||||||||||||||||||
Other comprehensive loss |
— |
— |
— |
— |
— |
(15,810 |
) |
— |
— |
(15,810 |
) |
||||||||||||||||||||||
Balance at December 31, 2014 |
433,421,677 |
$ |
4,334 |
(1,245,367 |
) |
$ |
(4,051 |
) |
$ |
1,529,096 |
$ |
(12,392 |
) |
$ |
(674,843 |
) |
$ |
(6,403 |
) |
$ |
835,741 |
||||||||||||
The accompanying Notes to Consolidated Financial Statements are an integral part of these statements.
78
OPKO Health, Inc. and Subsidiaries
CONSOLIDATED STATEMENTS OF EQUITY
(In thousands, except share and per share data)
For the years ended December 31, 2015, 2014, 2013 (continued)
Common Stock |
Treasury |
Additional
Paid-In
Capital
|
Accumulated Other
Comprehensive
Loss
|
Accumulated
Deficit
|
Noncontrolling
Interests
|
Total |
|||||||||||||||||||||||||||
Shares |
Dollars |
Shares |
Dollars |
||||||||||||||||||||||||||||||
Balance at December 31, 2014 |
433,421,677 |
$ |
4,334 |
(1,245,367 |
) |
$ |
(4,051 |
) |
$ |
1,529,096 |
$ |
(12,392 |
) |
$ |
(674,843 |
) |
$ |
(6,403 |
) |
$ |
835,741 |
||||||||||||
Equity-based compensation expense |
— |
— |
— |
— |
26,074 |
— |
— |
— |
26,074 |
||||||||||||||||||||||||
Exercise of Common Stock options and warrants |
24,467,806 |
245 |
— |
— |
25,675 |
— |
— |
— |
25,920 |
||||||||||||||||||||||||
Issuance of Common Stock for EirGen purchase |
2,420,487 |
24 |
— |
— |
33,572 |
— |
— |
— |
33,596 |
||||||||||||||||||||||||
Issuance of Common Stock for BRL purchase |
76,566,147 |
766 |
— |
— |
949,244 |
— |
— |
— |
950,010 |
||||||||||||||||||||||||
Issuance of Common Stock upon exchange of 2033 Senior Notes |
8,118,062 |
81 |
— |
— |
120,218 |
— |
— |
— |
120,299 |
||||||||||||||||||||||||
Issuance of Treasury Stock in connection with OPKO Health Europe’s Contingent Consideration |
— |
— |
125,000 |
406 |
1,406 |
— |
— |
— |
1,812 |
||||||||||||||||||||||||
Issuance of Common Stock for OPKO Renal earnout |
1,194,337 |
12 |
— |
— |
20,100 |
— |
— |
— |
20,112 |
||||||||||||||||||||||||
Net loss attributable to common shareholders |
— |
— |
— |
— |
— |
— |
(30,028 |
) |
— |
(30,028 |
) |
||||||||||||||||||||||
Deconsolidation of SciVac |
— |
— |
— |
— |
— |
— |
— |
6,403 |
6,403 |
||||||||||||||||||||||||
Other comprehensive loss |
— |
— |
— |
— |
— |
(10,145 |
) |
— |
— |
(10,145 |
) |
||||||||||||||||||||||
Balance at December 31, 2015 |
546,188,516 |
$ |
5,462 |
(1,120,367 |
) |
$ |
(3,645 |
) |
$ |
2,705,385 |
$ |
(22,537 |
) |
$ |
(704,871 |
) |
$ |
— |
$ |
1,979,794 |
|||||||||||||
The accompanying Notes to Consolidated Financial Statements are an integral part of these statements.
79
OPKO Health, Inc. and Subsidiaries
CONSOLIDATED STATEMENTS OF CASH FLOWS
(In thousands)
For the years ended December 31, |
|||||||||||
2015 |
2014 |
2013 |
|||||||||
Cash flows from operating activities: |
|||||||||||
Net loss |
$ |
(31,428 |
) |
$ |
(174,638 |
) |
$ |
(117,346 |
) |
||
Adjustments to reconcile net loss to net cash used in operating activities: |
|||||||||||
Depreciation and amortization |
42,248 |
14,927 |
15,216 |
||||||||
Non-cash interest on 2033 Senior Notes |
2,612 |
5,662 |
5,980 |
||||||||
Amortization of deferred financing costs |
1,212 |
2,007 |
1,170 |
||||||||
Losses from investments in investees |
7,105 |
3,587 |
11,456 |
||||||||
Equity-based compensation – employees and non-employees |
26,074 |
14,779 |
10,983 |
||||||||
Provision for bad debts |
24,548 |
646 |
979 |
||||||||
Provision for inventory obsolescence |
926 |
1,082 |
2,015 |
||||||||
Revenue from receipt of equity |
(140 |
) |
(240 |
) |
(12,740 |
) |
|||||
Realized gain (loss) on equity securities |
7,091 |
167 |
(29,881 |
) |
|||||||
Gain on conversion of 3.00% convertible senior notes |
(943 |
) |
(2,668 |
) |
(972 |
) |
|||||
Loss on sale of property, plant and equipment |
— |
— |
60 |
||||||||
Change in fair value of derivative instruments |
39,083 |
10,632 |
45,942 |
||||||||
In-process research and development |
— |
12,055 |
— |
||||||||
Change in fair value of contingent consideration |
5,050 |
24,446 |
6,947 |
||||||||
Gain on deconsolidation of SciVac |
(15,940 |
) |
— |
— |
|||||||
Deferred income tax (benefit) provision |
(123,536 |
) |
1,017 |
599 |
|||||||
Changes in assets and liabilities, net of the effects of acquisitions: |
|||||||||||
Accounts receivable |
(29,393 |
) |
(3,919 |
) |
754 |
||||||
Inventory |
(5,879 |
) |
(1,752 |
) |
1,892 |
||||||
Prepaid expenses and other current assets |
(4,391 |
) |
3,182 |
(1,131 |
) |
||||||
Other assets |
(305 |
) |
(3,378 |
) |
(544 |
) |
|||||
Accounts payable |
(18,122 |
) |
(3,852 |
) |
1,829 |
||||||
Foreign currency measurement |
979 |
945 |
(2,386 |
) |
|||||||
Deferred revenue |
227,671 |
— |
— |
||||||||
Accrued expenses and other liabilities |
9,502 |
4,934 |
3,525 |
||||||||
Net cash provided by (used in) operating activities |
164,024 |
(90,379 |
) |
(55,653 |
) |
||||||
Cash flows from investing activities: |
|||||||||||
Investments in investees |
(4,375 |
) |
(589 |
) |
(17,441 |
) |
|||||
Proceeds from sale of equity securities |
— |
1,331 |
30,556 |
||||||||
Acquisition of businesses, net of cash acquired |
(79,000 |
) |
(1,683 |
) |
20,528 |
||||||
Acquisition of intangible assets |
(5,000 |
) |
— |
— |
|||||||
Purchase of marketable securities |
— |
— |
(50,027 |
) |
|||||||
Maturities of short-term marketable securities |
— |
— |
50,027 |
||||||||
Proceeds from the sale of property, plant and equipment |
— |
— |
636 |
||||||||
Capital expenditures |
(10,846 |
) |
(4,734 |
) |
(3,962 |
) |
|||||
Net cash provided by (used in) investing activities |
(99,221 |
) |
(5,675 |
) |
30,317 |
||||||
Cash flows from financing activities: |
|||||||||||
Issuance of 2033 Senior Notes, net, including related parties |
— |
— |
170,184 |
||||||||
Payment of Series D dividends, including related parties |
— |
— |
(3,015 |
) |
|||||||
Proceeds from the exercise of Common Stock options and warrants |
25,921 |
12,928 |
23,425 |
||||||||
Cash from non-controlling interest |
100 |
2,696 |
— |
||||||||
Contingent consideration payments |
— |
(6,435 |
) |
(2,539 |
) |
||||||
Borrowings on lines of credit |
261,339 |
26,443 |
34,577 |
||||||||
Repayments of lines of credit |
(254,355 |
) |
(28,369 |
) |
(38,997 |
) |
|||||
Net cash provided by financing activities |
33,005 |
7,263 |
183,635 |
||||||||
Effect of exchange rate on cash and cash equivalents |
(1,117 |
) |
(100 |
) |
138 |
||||||
Net increase (decrease) in cash and cash equivalents |
96,691 |
(88,891 |
) |
158,437 |
|||||||
Cash and cash equivalents at beginning of period |
96,907 |
185,798 |
27,361 |
||||||||
Cash and cash equivalents at end of period |
$ |
193,598 |
$ |
96,907 |
$ |
185,798 |
|||||
SUPPLEMENTAL INFORMATION: |
|||||||||||
Interest paid |
$ |
4,572 |
$ |
6,276 |
$ |
3,407 |
|||||
Income taxes paid, net |
$ |
4,879 |
$ |
954 |
$ |
1,321 |
|||||
RXi common stock received |
$ |
— |
$ |
— |
$ |
12,500 |
|||||
Pharmsynthez common stock received |
$ |
— |
$ |
6,264 |
$ |
— |
|||||
Non-cash financing: |
|||||||||||
Assets acquired under capital leases |
|||||||||||
Shares issued upon the conversion of: |
|||||||||||
Series D Preferred Stock |
$ |
— |
$ |
— |
$ |
24,386 |
|||||
2033 Senior Notes |
$ |
120,299 |
$ |
95,665 |
$ |
20,839 |
|||||
Common Stock options and warrants, surrendered in net exercise |
$ |
14,369 |
$ |
3,494 |
$ |
815 |
|||||
Issuance of capital stock to acquire or contingent consideration settlement: |
|||||||||||
Bio-Reference Laboratories, Inc. |
$ |
950,148 |
$ |
— |
$ |
— |
|||||
EirGen Pharma Limited |
$ |
33,569 |
$ |
— |
$ |
— |
|||||
OPKO Biologics |
$ |
— |
$ |
— |
$ |
586,643 |
|||||
OPKO Renal |
$ |
20,113 |
$ |
21,155 |
$ |
146,902 |
|||||
OPKO Brazil |
$ |
— |
$ |
— |
$ |
436 |
|||||
OPKO Health Europe |
$ |
1,813 |
$ |
— |
$ |
4,404 |
|||||
OPKO Uruguay Ltda. |
$ |
— |
$ |
159 |
$ |
— |
|||||
Inspiro |
$ |
— |
$ |
8,566 |
$ |
— |
|||||
The accompanying Notes to Consolidated Financial Statements are an integral part of these statements.
80
OPKO Health, Inc. and Subsidiaries
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Note 1 Business and Organization
We are a diversified healthcare company that seeks to establish industry-leading positions in large and rapidly growing medical markets. Our diagnostics business includes Bio-Reference Laboratories, the nation’s third-largest clinical laboratory with a core genetic testing business and a 420-person sales force to drive growth and leverage new products, including the 4Kscore prostate cancer test and the Claros 1 in-office immunoassay platform. Our pharmaceutical business features Rayaldee, a treatment for secondary hyperparathyroidism (“SHPT”) in patients with stage 3 or 4 chronic kidney disease (“CKD”) and vitamin D insufficiency (March 29, 2016 PDUFA date) and VARUBI™ for chemotherapy-induced nausea and vomiting (launched by partner TESARO in November 2015). Our pharmaceutical business includes OPKO Biologics, which features hGH-CTP, a once-weekly human growth hormone injection (in Phase 3 and partnered with Pfizer), and a once-daily Factor VIIa drug for hemophilia (Phase 2a). We are incorporated in Delaware and our principal executive offices are located in leased offices in Miami, Florida.
In August 2015, we completed the acquisition of Bio-Reference, the third largest full service clinical laboratory in the United States, known for its innovative technological solutions and pioneering leadership in the areas of genomics and genetic sequencing. Holders of Bio-Reference common stock received 76,566,147 shares of OPKO Common Stock for the outstanding shares of Bio-Reference common stock. The transaction was valued at approximately $950.1 million, based on a closing price per share of our Common Stock of $12.38 as reported by the New York Stock Exchange on the closing date, or $34.05 per share of Bio-Reference common stock. Included in the transaction value is $2.3 million related to the value of replacement stock option awards attributable to pre-merger service.
Through our acquisition of Bio-Reference, we provide laboratory testing services, primarily to customers in the larger metropolitan areas across New York, New Jersey, Maryland, Pennsylvania, Delaware, Washington DC, Florida, California, Texas, Illinois and Massachusetts as well as to customers in a number of other states. We offer a comprehensive list of clinical diagnostic tests including blood and urine analysis, blood chemistry, hematology services, serology, radio-immuno analysis, toxicology (including drug screening), pap smears, tissue pathology (biopsies) and other tissue analysis. We perform cancer cytogenetic testing at our leased facilities in Elmwood Park, NJ, Smithtown, NY, Clarksburg, MD, Milford, MA, Miami, FL, and Campbell, CA and genetic testing at our leased facility in Gaithersburg, MD, as well as at our Elmwood Park facility. We perform cytology testing at our leased facilities Frederick, MD, Milford, MA, Columbus, OH, Houston, TX and at our Elmwood Park facility. We market our laboratory testing services directly to physicians, geneticists, hospitals, clinics, correctional and other health facilities.
In May 2015, we acquired all of the issued and outstanding shares of EirGen Pharma Limited (“EirGen”), a specialty pharmaceutical company incorporated in Ireland focused on the development and commercial supply of high potency, high barrier to entry pharmaceutical products, for $133.8 million in the aggregate. We acquired the outstanding shares of EirGen for approximately $100.2 million in cash and delivered 2,420,487 shares of our Common Stock valued at approximately $33.6 million based on the closing price per share of our Common Stock as reported by the New York Stock Exchange on the closing date of the acquisition, $13.88 per share.
We operate established pharmaceutical platforms in Ireland, Chile, Spain, and Mexico, which are generating revenue and which we expect to facilitate future market entry for our products currently in development. In addition, we have a development and commercial supply pharmaceutical company and a global supply chain operation and holding company in Ireland. We own a specialty active pharmaceutical ingredients (“APIs”) manufacturer in Israel, which we expect will facilitate the development of our pipeline of molecules and compounds for our molecular diagnostic and therapeutic products.
Our research and development activities are primarily performed at leased facilities in Jupiter and Miramar, Florida, Woburn, Massachusetts, Waterford, Ireland, Nes Ziona, Israel, and Barcelona, Spain.
81
Note 2 Summary of Significant Accounting Policies
Basis of presentation. The accompanying Consolidated Financial Statements have been prepared in accordance with accounting principles generally accepted in the U.S. and with the instructions to Form 10-K and of Regulation S-X.
Principles of consolidation. The accompanying Consolidated Financial Statements include the accounts of OPKO Health, Inc. and of our wholly-owned subsidiaries. All intercompany accounts and transactions are eliminated in consolidation.
Use of estimates. The preparation of financial statements in conformity with accounting principles generally accepted in the United States requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenues and expenses during the reporting period. Actual results could differ significantly from these estimates.
Cash and cash equivalents. Cash and cash equivalents include short-term, interest-bearing instruments with original maturities of 90 days or less at the date of purchase. We also consider all highly liquid investments with original maturities at the date of purchase of 90 days or less as cash equivalents. These investments include money markets, bank deposits, certificates of deposit and U.S. treasury securities.
Inventories. Inventories are valued at the lower of cost or market (net realizable value). Cost is determined by the first-in, first-out method. We consider such factors as the amount of inventory on hand, estimated time required to sell such inventories, remaining shelf-life, and current market conditions to determine whether inventories are stated at the lower of cost or market. Inventories at our diagnostics segment consist primarily of purchased laboratory supplies, which is used in our testing laboratories.
Pre-launch inventories. We may accumulate commercial quantities of certain product candidates prior to the date we anticipate that such products will receive final U.S. FDA approval. The accumulation of such pre-launch inventories involves the risk that such products may not be approved for marketing by the FDA on a timely basis, or ever. This risk notwithstanding, we may accumulate pre-launch inventories of certain products when such action is appropriate in relation to the commercial value of the product launch opportunity. In accordance with our policy, this pre-launch inventory is expensed. At December 31, 2015 and 2014, there were no pre-launch inventories.
Goodwill and intangible assets. Goodwill represents the difference between the purchase price and the estimated fair value of the net assets acquired when accounted for by the acquisition method of accounting and arose from our acquisitions. Refer to Note 5. Goodwill, in-process research and development (“IPR&D”) and other intangible assets acquired in business combinations, licensing and other transactions at December 31, 2015 and 2014, were $2.2 billion and $1.1 billion, respectively.
Assets acquired and liabilities assumed in business combinations, licensing and other transactions are generally recognized at the date of acquisition at their respective fair values. We determined the fair value of intangible assets, including IPR&D, using the “income method.”
Goodwill is tested at least annually for impairment, or when events or changes in circumstances indicate that the carrying amount of such assets may not be recoverable, by assessing qualitative factors or performing a quantitative analysis in determining whether it is more likely than not that its fair value exceeds the carrying value.
Intangible assets are tested for impairment whenever events or changes in circumstances indicate that the carrying amount of such assets may not be recoverable, although IPR&D is required to be tested at least annually until the project is completed or abandoned. Upon obtaining regulatory approval, the IPR&D asset is then accounted for as a finite-lived intangible asset and amortized on a straight-line basis over its estimated useful life. If the project is abandoned, the IPR&D asset is charged to expense.
We amortize intangible assets with definite lives on a straight-line basis over their estimated useful lives, currently ranging from 3 to 20 years. We use the straight-line method of amortization as there is no reliably determinable pattern in which the economic benefits of our intangible assets are consumed or otherwise used up. Amortization expense was $28.0 million, $10.9 million and $11.1 million for the years ended December 31, 2015, 2014 and 2013, respectively. Amortization expense from operations for our intangible assets is expected to be $51.3 million, $50.8 million, $47.7 million, $44.2 million and $42.9 million for the years ended December 2016, 2017, 2018, 2019 and 2020, respectively.
Fair value measurements. The carrying amounts of our cash and cash equivalents, accounts receivable, accounts payable and short-term debt approximate their fair value due to the short-term maturities of these instruments. Investments that are considered available for sale as of December 31, 2015 and 2014 are carried at fair value.
82
In evaluating the fair value information, considerable judgment is required to interpret the market data used to develop the estimates. The use of different market assumptions and/or different valuation techniques may have a material effect on the estimated fair value amounts. Accordingly, the estimates of fair value presented herein may not be indicative of the amounts that could be realized in a current market exchange. Refer to Note 17.
Contingent consideration. Each period we revalue the contingent consideration obligations associated with certain prior acquisitions to their fair value and record increases in the fair value as contingent consideration expense and decreases in the fair value as a reduction in contingent consideration expense. Changes in contingent consideration result from changes in the assumptions regarding probabilities of successful achievement of related milestones, the estimated timing in which the milestones are achieved and the discount rate used to estimate the fair value of the liability. Contingent consideration may change significantly as our development programs progress, revenue estimates evolve and additional data is obtained, impacting our assumptions. The assumptions used in estimating fair value require significant judgment. The use of different assumptions and judgments could result in a materially different estimate of fair value which may have a material impact on our results from operations and financial position.
Derivative financial instruments. We record derivative financial instruments on our Consolidated Balance Sheet at their fair value and recognize the changes in the fair value in our Consolidated Statement of Operations when they occur, the only exception being derivatives that qualify as hedges. For the derivative instrument to qualify as a hedge, we are required to meet strict hedge effectiveness and contemporaneous documentation requirements at the initiation of the hedge and assess the hedge effectiveness on an ongoing basis over the life of the hedge. At December 31, 2015 and 2014, our forward contracts for inventory purchases did not meet the documentation requirements to be designated as hedges. Accordingly, we recognize all changes in the fair values of our derivatives instruments, net, in our Consolidated Statement of Operations. Refer to Note 18.
Property, Plant and Equipment. Property, plant and equipment are recorded at cost. Depreciation is provided using the straight-line method over the estimated useful lives of the assets, generally five to ten years and includes amortization expense for assets capitalized under capital leases. The estimated useful lives by asset class are as follows: software - 3 years, machinery, medical and other equipment - 5-8 years, furniture and fixtures - 5-10 years, leasehold improvements - the lesser of their useful life or the lease term, buildings and improvements - 10-40 years, automobiles and aircraft - 5-7 years. Expenditures for repairs and maintenance are charged to expense as incurred. Depreciation expense was $14.2 million, $4.0 million and $4.1 million for the years ended December 31, 2015, 2014 and 2013, respectively. Assets held under capital leases are included within Property, plant and equipment, net in our Consolidated Balance Sheet and are amortized over the shorter of their useful lives or the term of their related leases.
Impairment of Long-Lived Assets. Long-lived assets, such as property and equipment, are reviewed for impairment whenever events or changes in circumstances indicate that the carrying amount of an asset may not be recoverable. Recoverability of assets to be held and used is measured by a comparison of the carrying amount of an asset to estimated undiscounted future cash flows expected to be generated by the asset. If the carrying amount of an asset exceeds its estimated future cash flows, then an impairment charge is recognized for the amount by which the carrying amount of the asset exceeds the fair value, or carrying amount for cost basis assets, of the asset.
Income Taxes. Income taxes are accounted for under the asset-and-liability method. Deferred tax assets and liabilities are recognized for the future tax consequences attributable to differences between the financial statement carrying amounts of existing assets and liabilities and the respective tax bases and operating loss and tax credit carryforwards. Deferred tax assets and liabilities are measured using enacted tax rates expected to apply to taxable income in the years in which those temporary differences are expected to be recovered or settled. The effect on deferred tax assets and liabilities of a change in tax rates is recognized in operations in the period that includes the enactment date. We periodically evaluate the realizability of our net deferred tax assets. Our tax accruals are analyzed periodically and adjustments are made as events occur to warrant such adjustment.
Income tax benefit for the year ended December 31, 2015 was primarily due to a $93.4 million release of a valuation allowance on our U.S. deferred tax assets due to a change in the assessment of recoverability following the merger with Bio-Reference in August 2015. This was partially offset by expense recognized on taxable income from the Pfizer Transaction during the year ended December 31, 2015. Refer to Note 14 for a discussion of the Pfizer Transaction.
Included in income tax benefit is an accrual of $2.3 million related to uncertain tax positions involving income recognition. We recognize that local tax law is inherently complex and the local taxing authorities may not agree with certain tax positions taken. Consequently, it is reasonably possible that the ultimate resolution of tax matters in any jurisdiction may be significantly more or less than estimated. We evaluated the estimated tax exposure for a range of current likely outcomes to be from $0 to approximately $50.0 million and recorded our accrual to reflect our best expectation of ultimate resolution.
83
Revenue recognition. Revenue for laboratory services is recognized at the time test results are reported, which approximates when services are provided. Services are provided to patients covered by various third-party payer programs including various managed care organizations, as well as the Medicare and Medicaid programs. Billings for services under third-party payer programs are included in revenue net of allowances for contractual discounts and allowances for differences between the amounts billed and estimated program payment amounts. Adjustments to the estimated payment amounts based on final settlement with the programs are recorded upon settlement as an adjustment to revenue. For the years ended December 31, 2015 and 2014, approximately 9% and 5%, respectively, of our revenues were derived directly from the Medicare and Medicaid programs. The increase in revenues from laboratory services, including revenue from Medicare and Medicaid programs, is due to the acquisition of Bio-Reference in August 2015.
Generally, we recognize revenue from product sales when goods are shipped and title and risk of loss transfer to our customers. Our estimates for sales returns and allowances are based upon the historical patterns of product returns and allowances taken, matched against the sales from which they originated, and management’s evaluation of specific factors that may increase or decrease the risk of product returns.
Revenue from transfer of intellectual property includes revenue related to the sale, license or transfer of intellectual property such as upfront license payments, license fees and milestone payments received through our license, collaboration and commercialization agreements. We analyze our multiple-element arrangements to determine whether the elements can be separated and accounted for individually as separate units of accounting.
Non-refundable license fees for the out-license of our technology are recognized depending on the provisions of each agreement. We recognize non-refundable upfront license payments as revenue upon receipt if the license has standalone value and qualifies for treatment as a separate unit of accounting under multiple-element arrangement guidance. License fees with ongoing involvement or performance obligations that do not have standalone value are recorded as deferred revenue, included in Accrued expenses or Other long-term liabilities, when received and generally are recognized ratably over the period of such performance obligations only after both the license period has commenced and we have delivered the technology.
The assessment of our obligations and related performance periods requires significant management judgment. If an agreement contains research and development obligations, the relevant time period for the research and development phase is based on management estimates and could vary depending on the outcome of clinical trials and the regulatory approval process. Such changes could materially impact the revenue recognized, and as a result, management reviews the estimates related to the relevant time period of research and development on a quarterly basis. For the years ended December 31, 2015, 2014 and 2013 we recorded $81.9 million, $5.5 million and $16.7 million of revenue from the transfer of intellectual property, respectively. For the year ended December 31, 2015, revenue from the transfer of intellectual property included $15.0 million related to a milestone payment that TESARO, Inc. (“TESARO”) paid us under our license agreement with them and $65.5 million related to the Pfizer Transaction. Refer to Note 14. For the year ended December 31, 2014, $5.0 million related to a milestone payment that TESARO paid us under our license agreement with them. For the year ended December 31, 2013, $12.5 million related to the sale of substantially all of our assets in the field of RNA interference to RXi Pharmaceuticals Corporation (“RXi”) and $3.8 million related to the rights granted to OAO Pharmsynthez (“Pharmsynthez”) for certain technologies.
Revenue from milestone payments related to arrangements under which we have continuing performance obligations are recognized as Revenue from transfer of intellectual property upon achievement of the milestone only if all of the following conditions are met: the milestone payments are non-refundable; there was substantive uncertainty at the date of entering into the arrangement that the milestone would be achieved; the milestone is commensurate with either our performance to achieve the milestone or the enhancement of the value of the delivered item by us; the milestone relates solely to past performance; and the amount of the milestone is reasonable in relation to the effort expended or the risk associated with the achievement of the milestone. If any of these conditions are not met, the milestone payments are not considered to be substantive and are, therefore, deferred and recognized as Revenue from transfer of intellectual property over the term of the arrangement as we complete our performance obligations.
Total deferred revenue included in Accrued expenses and Other long-term liabilities was $232.9 million and $6.7 million at December 31, 2015 and 2014, respectively. The deferred revenue balance at December 31, 2015 relates primarily to the Pfizer Transaction. Refer to Note 14.
Concentration of Credit Risk and Allowance for doubtful accounts. Financial instruments that potentially subject us to concentrations of credit risk consist primarily of accounts receivable. Substantially all of our accounts receivable are with companies in the health care industry and individuals. However, credit risk is limited due to the number of our clients as well as their dispersion across many different geographic regions.
While we have receivables due from federal and state governmental agencies, we do not believe that such receivables represent a credit risk since the related health care programs are funded by federal and state governments, and payment is
84
primarily dependent upon submitting appropriate documentation. Accounts receivable balances (prior to allowance for doubtful accounts and net of contractual adjustments) from Medicare and Medicaid were $26.1 million and $0.6 million at December 31, 2015 and 2014, respectively.
The portion of our accounts receivable due from patients comprises the largest portion of credit risk. At December 31, 2015 and 2014, receivables due from patients represent approximately 7.5% and 0.5% of our consolidated accounts receivable (prior to allowance for doubtful accounts and net of contractual adjustments).
We assess the collectability of accounts receivable balances by considering factors such as historical collection experience, customer credit worthiness, the age of accounts receivable balances, regulatory changes and current economic conditions and trends that may affect a customer’s ability to pay. Actual results could differ from those estimates. Our reported net income (loss) is directly affected by our estimate of the collectability of accounts receivable. The allowance for doubtful accounts recognized in our Consolidated Balance Sheets was $25.2 million and $1.9 million at December 31, 2015 and 2014, respectively.
Equity-based compensation. We measure the cost of employee services received in exchange for an award of equity instruments based on the grant-date fair value of the award. That cost is recognized in the Consolidated Statement of Operations over the period during which an employee is required to provide service in exchange for the award. We record excess tax benefits, realized from the exercise of stock options as a financing cash inflow and as a reduction of taxes paid in cash flow from operations. Equity-based compensation arrangements to non-employees are recorded at their fair value on the measurement date. The measurement of equity-based compensation to non-employees is subject to periodic adjustment as the underlying equity instruments vest. During the years ended December 31, 2015, 2014 and 2013, we recorded $26.1 million, $14.8 million and $11.0 million, respectively, of equity-based compensation expense.
Research and development expenses. Research and development expenses include external and internal expenses, partially offset by third-party grants and fundings arising from collaboration agreements. External expenses include clinical and non-clinical activities performed by contract research organizations, lab services, purchases of drug and diagnostic product materials and manufacturing development costs. Research and development employee-related expenses include salaries, benefits and stock-based compensation expense. Other internal research and development expenses are incurred to support overall research and development activities and include expenses related to general overhead and facilities. We expense these costs in the period in which they are incurred. We estimate our liabilities for research and development expenses in order to match the recognition of expenses to the period in which the actual services are received. As such, accrued liabilities related to third party research and development activities are recognized based upon our estimate of services received and degree of completion of the services in accordance with the specific third party contract.
We record expense for in-process research and development projects acquired as asset acquisitions which have not reached technological feasibility and which have no alternative future use. For in-process research and development projects acquired in business combinations, the in-process research and development project is capitalized and evaluated for impairment until the development process has been completed. Once the development process has been completed the asset will be amortized over its remaining useful life.
Segment reporting. Our chief operating decision-maker (“CODM”) is Phillip Frost, M.D., our Chairman and Chief Executive Officer. Our CODM reviews our operating results and operating plans and makes resource allocation decisions on a Company-wide or aggregate basis. We currently manage our operations in two reportable segments, pharmaceutical and diagnostics. The pharmaceutical segment consists of our pharmaceutical operations we acquired in Chile, Mexico, Ireland, Israel and Spain and our pharmaceutical research and development. The diagnostics segment primarily consists of our clinical laboratory operations we acquired through the acquisitions of Bio-Reference and OPKO Lab and our point-of-care operations. There are no significant inter-segment sales. We evaluate the performance of each segment based on operating profit or loss. There is no inter-segment allocation of interest expense and income taxes.
Shipping and Handling Costs. We do not charge customers for shipping and handling costs. Shipping and handling costs are classified as Cost of revenues in the Consolidated Statements of Operations.
Foreign Currency Translation. The financial statements of certain of our foreign operations are measured using the local currency as the functional currency. The local currency assets and liabilities are generally translated at the rate of exchange to the United States (“U.S.”) dollar on the balance sheet date and the local currency revenues and expenses are translated at average rates of exchange to the U.S. dollar during the reporting periods. Foreign currency transaction gains (losses) have been reflected as a component of Other income (expense), net within the Consolidated Statements of Operations and foreign currency translation gains (losses) have been included as a component of the Consolidated Statements of Comprehensive Loss. During the years ended December 31, 2015, 2014 and 2013, we recorded $(2.4) million, $(4.8) million and $(0.3) million, respectively of transaction gains (losses).
85
Variable interest entities. The consolidation of variable interest entities (“VIE”) is required when an enterprise has a controlling financial interest. A controlling financial interest in a VIE will have both of the following characteristics: (a) the power to direct the activities of a VIE that most significantly impact the VIE’s economic performance and (b) the obligation to absorb losses of the VIE that could potentially be significant to the VIE. In July 2015, we deconsolidated SciVac Therapeutics Inc., (“STI”), and account for our retained interest in STI as an equity method investment. Refer to Note 4.
Investments. We have made strategic investments in development stage and emerging companies. We record these investments as equity method investments or investments available for sale based on our percentage of ownership and whether we have significant influence over the operations of the investees. Investments for which it is not practical to estimate fair value and which we do not have significant influence are accounted for as cost method investments. For investments classified under the equity method of accounting, we record our proportionate share of their losses in Losses from investments in investees in our Consolidated Statement of Operations. Refer to Note 4. For investments classified as available for sale, we record changes in their fair value as unrealized gain or loss in Other comprehensive income (loss) based on their closing price per share at the end of each reporting period. Refer to Note 4.
Recent accounting pronouncements. In May 2014, the FASB issued Accounting Standards Update (“ASU”), ASU No. 2014-09, “Revenue from Contracts with Customers.” ASU No. 2014-09 clarifies the principles for recognizing revenue and develops a common revenue standard for GAAP and International Financial Reporting Standards that removes inconsistencies and weaknesses in revenue requirements, provides a more robust framework for addressing revenue issues, improves comparability of revenue recognition practices across entities, industries, jurisdictions, and capital markets, provides more useful information to users of financial statements through improved disclosure requirements and simplifies the preparation of financial statements by reducing the number of requirements to which an entity must refer. ASU No. 2014-09 is effective for fiscal years, and interim periods within those years, beginning after December 15, 2017. Companies can choose to apply the ASU using either the full retrospective approach or a modified retrospective approach. We are currently evaluating both methods of adoption and the impact that the adoption of this ASU will have on our Consolidated Financial Statements.
In June 2014, the FASB issued ASU No. 2014-12, “Accounting for Share-Based Payments When the Terms of an Award Provide That a Performance Target Could Be Achieved after the Requisite Service Period (a consensus of the FASB Emerging Issues Task Force).” ASU No. 2014-12 requires that a performance target that affects vesting and that could be achieved after the requisite service period be treated as a performance condition. ASU No. 2014-12 is effective for fiscal years, and interim periods within those years, beginning after December 15, 2015. Earlier adoption is permitted. The amendments can be applied either prospectively to all awards granted or modified after the effective date or retrospectively to all awards with performance targets that are outstanding as of the beginning of the earliest annual period presented in the financial statements and to all new or modified awards. We expect to apply the ASU prospectively and do not expect the adoption to have an impact on our Consolidated Financial Statements.
In August 2014, the FASB issued ASU No. 2014-15, “Disclosure of Uncertainties about an Entity’s Ability to Continue as a Going Concern,” to provide guidance on management’s responsibility in evaluating whether there is substantial doubt about a company’s ability to continue as a going concern and to provide related footnote disclosures. ASU 2014-15 is effective for annual periods ending after December 15, 2016 with early adoption permitted. We do not believe the impact of our pending adoption of ASU 2014-15 on our Consolidated Financial Statements will be material.
In February 2015, the FASB issued ASU No. 2015-02, “Consolidation (Topic 810): Amendments to the Consolidation Analysis,” which amends current consolidation guidance including changes to both the variable and voting interest models used by companies to evaluate whether an entity should be consolidated. The requirements from ASU 2015-02 are effective for interim and annual periods beginning after December 15, 2015, with early adoption permitted. We do not believe the impact of our pending adoption of ASU 2015-02 on our Consolidated Financial Statements will be material.
In July 2015, the FASB issued ASU No. 2015-11, “Inventory (Topic 330): Simplifying the Measurement of Inventory,” which changes the measurement principle for entities that do not measure inventory using the last-in, first-out (“LIFO”) or retail inventory method from the lower of cost or market to lower of cost and net realizable value. ASU 2015-11 is effective for fiscal years beginning after December 15, 2016, including interim periods within those fiscal years, with early adoption permitted. We are currently evaluating the impact of this new guidance on our Consolidated Financial Statements.
In September 2015, the FASB issued ASU No. 2015-16, “Business Combinations (Topic 805): Simplifying the Accounting for Measurement-Period Adjustments,” which replaces the requirement that an acquirer in a business combination account for measurement period adjustments retrospectively with a requirement that an acquirer recognize adjustments to the provisional amounts that are identified during the measurement period in the reporting period in which the adjustment amounts are determined. ASU 2015-16 requires that the acquirer record, in the same period’s financial statements, the effect on earnings of changes in depreciation, amortization, or other income effects, if any, as a result of the change to the provisional amounts,
86
calculated as if the accounting had been completed at the acquisition date. ASU 2015-16 is effective for fiscal years beginning after December 15, 2015, including interim periods within those fiscal years. The guidance is to be applied prospectively to adjustments to provisional amounts that occur after the effective date of the guidance, with earlier application permitted for financial statements that have not been issued. Our early adoption of ASU 2015-16 in the third quarter of 2015 did not have a material impact on our Consolidated Financial Statements.
In November 2015, the FASB issued ASU No. 2015-17, “Income Taxes (Topic 740): Balance Sheet Classification of Deferred Taxes,” which requires deferred tax liabilities and assets to be classified as noncurrent in a classified statement of financial position. ASU 2015-17 is effective for financial statements issued for annual periods beginning after December 15, 2016, and interim periods within those annual periods. Earlier application is permitted for all entities as of the beginning of an interim or annual reporting period. We adopted the provisions of this ASU prospectively in the fourth quarter of 2015, and did not retrospectively adjust the prior periods. The adoption of this ASU will simplify the presentation of deferred income taxes and reduce complexity without decreasing the usefulness of information provided to users of financial statements. The adoption of ASU 2015-17 did not have a significant impact on our financial position, results of operations and cash flows.
Note 3 Loss Per Share
Basic loss per share is computed by dividing our net loss by the weighted average number of shares outstanding during the period. For diluted earnings per share, the dilutive impact of stock options, warrants and bifurcated conversion option of the 2033 Senior Notes is determined by applying the “treasury stock” method. In the periods in which their effect would be antidilutive, no effect has been given to outstanding options, warrants or the potentially dilutive shares issuable pursuant to the 2033 Senior Notes (defined in Note 6) in the dilutive computation.
A total of 14,269,717, 28,456,149 and 32,105,859 potential shares of Common Stock have been excluded from the calculation of diluted net loss per share for the years ended December 31, 2015, 2014 and 2013, respectively, because their inclusion would be antidilutive.
During the year ended December 31, 2015, 25,686,153 Common Stock options and Common Stock warrants to purchase shares of our Common Stock were exercised, resulting in the issuance of 24,466,106 shares of Common Stock. Of the 25,686,153 Common Stock options and Common Stock warrants exercised, 1,220,047 shares of Common Stock were surrendered in lieu of a cash payment via the net exercise feature of the agreements.
During the year ended December 31, 2014, 5,787,983 Common Stock options and Common Stock warrants to purchase shares of our Common Stock were exercised, resulting in the issuance of 5,392,741 shares of Common Stock. Of the 5,787,983 Common Stock options and Common Stock warrants exercised, 426 shares of Common Stock were surrendered in lieu of a cash payment via the net exercise feature of the agreements.
During the year ended December 31, 2013, 10,881,570 Common Stock options and Common Stock warrants to purchase shares of our Common Stock were exercised, resulting in the issuance of 10,732,745 shares of Common Stock. Of the 10,881,570 Common Stock options and Common Stock warrants exercised, 148,825 shares of Common Stock were surrendered in lieu of a cash payment via the net exercise feature of the agreements.
Note 4 Acquisitions, Investments and Licenses
Bio-Reference acquisition
In August 2015, we completed the acquisition of Bio-Reference, the third largest full service clinical laboratory in the United States, known for its innovative technological solutions and pioneering leadership in the areas of genomics and genetic sequencing. Holders of Bio-Reference common stock received 76,566,147 shares of OPKO Common Stock for the outstanding shares of Bio-Reference common stock. The transaction was valued at approximately $950.1 million, based on a closing price per share of our Common Stock of $12.38 as reported by the New York Stock Exchange on the closing date, or $34.05 per share of Bio-Reference common stock. Included in the transaction value is $2.3 million related to the value of replacement stock option awards attributable to pre-merger service.
The following table summarizes the preliminary purchase price allocation and the estimated fair value of the net assets acquired and liabilities assumed in the acquisition of Bio-Reference at the date of acquisition. The purchase price allocation for Bio-Reference is preliminary pending completion of the fair value analysis of acquired assets and liabilities:
87
(In thousands) |
Bio-Reference |
|||
Purchase price: |
||||
Value of OPKO Common Stock issued to Bio-Reference shareholders |
$ |
947,889 |
||
Value of replacement stock options awards to holders of Bio-Reference stock options |
2,259 |
|||
Total purchase price |
$ |
950,148 |
||
Preliminary value of assets acquired and liabilities assumed: |
||||
Current assets |
||||
Cash and cash equivalents |
$ |
15,800 |
||
Accounts receivable |
168,164 |
|||
Inventory |
19,674 |
|||
Other current assets, principally deferred tax assets |
61,135 |
|||
Total current assets |
264,773 |
|||
Property, plant and equipment |
112,457 |
|||
Intangible assets: |
||||
Trade name |
47,100 |
|||
Customer relationships |
395,200 |
|||
Technology |
100,600 |
|||
Total intangible assets |
542,900 |
|||
Goodwill |
441,158 |
|||
Investments |
5,326 |
|||
Other assets |
13,265 |
|||
Total assets |
1,379,879 |
|||
Accounts payable |
(77,908 |
) |
||
Accrued expenses |
(30,848 |
) |
||
Income taxes payable |
(437 |
) |
||
Lines of credit and notes payable |
(65,701 |
) |
||
Capital lease obligations |
(18,293 |
) |
||
Deferred tax liability (non-current) |
(236,544 |
) |
||
Total purchase price |
$ |
950,148 |
||
During the fourth quarter of 2015, we continued to finalize our purchase price allocation during the measurement period and obtained new fair value information related to certain assets acquired and liabilities assumed of Bio-Reference. As a result, in the fourth quarter of 2015 we adjusted the purchase price allocation initially recorded in the third quarter of 2015 by increasing accounts receivable by $5.2 million, decreasing Inventory by $0.2 million, increasing Other current assets by $7.0 million, increasing Property, plant and equipment by $6.2 million, decreasing intangible assets by $6.9 million, decreasing Goodwill by $31.6 million, increasing Other assets (long-term) by $1.1 million, decreasing Accounts payable by $1.5 million, increasing accrued expenses by $1.6 million, decreasing Income taxes payable by $20.0 million and increasing Deferred tax liability by $0.5 million. These adjustments did not have a significant impact on our fourth quarter results of operations or cash flows.
Goodwill from the acquisition of Bio-Reference principally relates to intangible assets that do not qualify for separate recognition (for instance, Bio-Reference’s assembled workforce), our expectation to develop and market new products, and the deferred tax liability generated as a result of the transaction. Goodwill is not tax deductible for income tax purposes and was assigned to the diagnostics reporting segment.
Revenue and Net loss in the Consolidated Statement of Operations for the year ended December 31, 2015 includes revenue and net income of Bio-Reference from the date of acquisition to December 31, 2015 of $321.9 million and $3.2 million, respectively.
88
The preliminary amortization periods for intangible assets acquired are 5 years for trade name, 10-20 years for customer relationships, 8-12 years for technology and 3 years for internally developed software.
We recognized $6.2 million of acquisition related costs for the acquisition of Bio-Reference that were expensed in the current period as a component of Selling, general and administrative expense.
Pro forma disclosure for Bio-Reference acquisition
The pro forma information has been prepared utilizing period ends that differ by less than 93 days, as permitted by Regulation S-X. We are a registrant with a fiscal year that ends on December 31 and Bio-Reference was a registrant with a fiscal year that ended on October 31. The pro forma results for the years ended December 31, 2015 and 2014 combines the results of operations of OPKO and Bio-Reference, giving effect to the merger as if it occurred on January 1, 2014, and are based on the individual consolidated statement of operations of OPKO as of December 31, 2015 and 2014 and Bio-Reference as of October 31, 2015 and 2014.
For the year ended December 31, |
||
(In thousands) |
2015 |
2014 |
Revenues |
$1,052,462 |
$923,407 |
Net loss |
(19,456) |
(140,854) |
Net loss attributable to common shareholders |
(18,055) |
(137,881) |
The pro forma financial information is presented for information purposes only. The financial information may not necessarily reflect our future results of operations or what the results of operations would have been had we owned and operated Bio-Reference as of the beginning of the period presented.
EirGen Pharma Limited acquisition
In May 2015, we acquired all of the issued and outstanding shares of EirGen, a specialty pharmaceutical company incorporated in Ireland focused on the development and commercial supply of high potency, high barrier to entry pharmaceutical products, for $133.8 million in the aggregate. We acquired the outstanding shares of EirGen for approximately $100.2 million in cash and delivered 2,420,487 shares of our Common Stock valued at approximately $33.6 million based on the closing price per share of our Common Stock as reported by the New York Stock Exchange on the closing date of the acquisition, $13.88 per share.
89
The following table summarizes the preliminary purchase price allocation and the estimated fair value of the net assets acquired and liabilities assumed in the acquisition of EirGen at the date of acquisition. The purchase price allocation for EirGen is preliminary pending completion of the fair value analysis of acquired assets and liabilities:
(In thousands) |
EirGen |
|||
Current assets (1)
|
$ |
11,795 |
||
Intangible assets: |
||||
IPR&D assets |
560 |
|||
Customer relationships |
34,155 |
|||
Currently marketed products |
3,919 |
|||
Total intangible assets |
38,634 |
|||
Goodwill |
83,373 |
|||
Property, plant and equipment |
8,117 |
|||
Other assets |
1,232 |
|||
Accounts payable and other liabilities |
(6,254 |
) |
||
Deferred tax liability |
(3,131 |
) |
||
Total purchase price |
$ |
133,766 |
||
(1)Current assets include cash, accounts receivable, inventory and other assets of $5.5 million, $2.7 million, $2.2 million and $1.4 million, respectively, related to the EirGen acquisition. The fair value of the accounts receivable equals the gross contractual amount at the date of acquisition.
During the fourth quarter of 2015, we continued to finalize our purchase price allocation during the measurement period and obtained new fair value information related to certain assets acquired of EirGen. As a result, in the fourth quarter of 2015 we adjusted the purchase price allocation initially recorded in the third quarter of 2015 by decreasing IPR&D assets by $19.0 million, increasing Goodwill by $16.6 million and decreasing Deferred tax liability by $2.5 million.
Goodwill from the acquisition of EirGen principally relates to intangible assets that do not qualify for separate recognition (for instance, EirGen’s assembled workforce), our expectation to develop and market new products, and the deferred tax liability generated as a result of this being a partial stock transaction. Goodwill is not tax deductible for income tax purposes and was assigned to the pharmaceutical reporting segment.
Revenue and Net loss in the Consolidated Statement of Operations for the year ended December 31, 2015 includes revenue and net income of EirGen from the date of acquisition to December 31, 2015 of $13.5 million and $1.4 million, respectively.
Our IPR&D assets will not be amortized until the underlying development programs are completed. Upon obtaining regulatory approval, the IPR&D assets are then accounted for as finite-lived intangible assets and amortized on a straight-line basis over its estimated useful life. We amortize intangible assets with definite lives on a straight-line basis over their estimated useful lives, currently ranging from 3 to 20 years.
We recognized $0.5 million of acquisition related costs for the acquisition of EirGen that were expensed in the current period as a component of Selling, general and administrative expense.
Pro forma disclosure for EirGen acquisition
The following table includes the pro forma results for the years ended December 31, 2015 and 2014 of the combined companies as though the acquisition of EirGen had been completed as of the beginning of the period presented.
90
For the year ended December 31, |
||
(In thousands) |
2015 |
2014 |
Revenues |
$495,993 |
$105,973 |
Net loss |
(32,481) |
(176,563) |
Net loss attributable to common shareholders |
(31,081) |
(173,590) |
The pro forma financial information is presented for information purposes only. The unaudited pro forma financial information may not necessarily reflect our future results of operations or what the results of operations would have been had we owned and operated EirGen as of the beginning of the period presented.
Inspiro Medical Ltd. acquisition
In May 2014, we acquired 100% of the issued and outstanding share capital of Inspiro Medical Ltd. (“Inspiro”), an Israeli medical device company developing a new platform to deliver small molecule drugs such as corticosteroids and beta agonists and larger molecules to treat respiratory diseases.
In connection with the transaction, we paid $1.5 million in cash and delivered 999,556 shares of our Common Stock valued at $8.6 million.
Inspiro’s Inspiromatic is a “smart” easy-to-use dry powder inhaler with several advantages over existing devices. We anticipate that this innovative device will play a valuable role in the improvement of therapy for asthma, chronic obstructive pulmonary disease, cystic fibrosis and other respiratory diseases. We recorded the transaction as an asset acquisition and recorded the assets and liabilities at fair value. As the asset had no alternative future use, we recorded $10.1 million of acquired in-process research and development expenses. We record expense for in-process research and development projects accounted for as asset acquisitions which have not reached technological feasibility and which have no alternative future use.
Investments
The following table reflects the accounting method, carrying value and underlying equity in net assets of our unconsolidated investments as of December 31, 2015:
(in thousands) |
||||||||
Investment type |
Investment Carrying Value |
Underlying Equity in Net Assets |
||||||
Equity method investments |
$ |
24,495 |
$ |
24,488 |
||||
Variable interest entity, equity method |
1,268 |
91 |
||||||
Available for sale investments |
3,615 |
|||||||
Warrants and options |
5,338 |
|||||||
Total carrying value of investments |
$ |
34,716 |
||||||
Equity Method Investments
Our equity method investments consist of investments in Pharmsynthez (ownership 17%), Cocrystal Pharma, Inc. (“COCP”) (8%), Sevion Therapeutics, Inc. (“Sevion”) (3%), Non-Invasive Monitoring Systems, Inc. (1%), Neovasc Inc. (4%), STI (25%) and InCellDx, Inc. (27%). The total assets, liabilities, and net losses of our equity method investees as of and for the years ended December 31, 2015 were $383.1 million, $61.6 million, and $73.3 million, respectively. We have determined that we and/or our related parties can significantly influence the success of our equity method investments through our board representation and voting power. Accordingly, we account for our investment in these entities under the equity method. For investments classified under the equity method of accounting, we record our proportionate share of their losses in Loss from investments in investees in our Consolidated Statement of Operations. The aggregate value of our equity method investments based on the quoted market price of their common stock and the number of shares held by us as of December 31, 2015 is $89.6 million.
Available for Sale Investments
Our available for sale investments consist of investments in RXi Pharmaceuticals Corporation (“RXi”) (ownership 3%), ChromaDex Corporation (2%), MabVax Therapeutics Holdings, Inc. (“MabVax”) (1%) and ARNO Therapeutics, Inc. (“ARNO”) (4%). We have determined that our ownership, along with that of our related parties, does not provide us with significant influence over the operations of our available for sale investments. Accordingly, we account for our investment in these entities as available
91
for sale, and we record changes in these investments as an unrealized gain or loss in Other comprehensive income (loss) each reporting period.
Based on our evaluation of the value of our investment in RXi, including RXi’s decreasing stock price during the year ended December 31, 2015, we determined that the decline in fair value of our RXi common shares was other-than-temporary and recorded an impairment charge of $7.3 million in Other income (expense), net in our Consolidated Statement of Operations for the year ended December 31, 2015 to write our investment in RXi common shares down to its fair value of $0.9 million as of December 31, 2015. Based on our evaluation of the value of our investment in ARNO, including ARNO’s decreasing stock price during the year ended December 31, 2014, we determined that the decline in fair value of our ARNO common shares was other-than-temporary and recorded an impairment charge of $1.4 million in Other income (expense), net in our Consolidated Statement of Operations for the year ended December 31, 2014 to write our investment in ARNO common shares down to its fair value of $0.6 million as of December 31, 2014. Refer to Note 17 for further discussion of the fair value of our available for sale investments.
Sales of Investments
Gains (losses) included in earnings from sales of our investments for the years ended December 31, 2015, 2014 and 2013 were $0.0 million, $1.3 million and $29.9 million, respectively, and were recorded in Other income (expense), net in our Consolidated Statement of Operations. The cost of securities sold is based on the specific identification method.
Warrants and Options
In addition to our equity method investments and available for sale investments, we hold options to purchase 1.0 million additional shares of Neovasc, which are fully vested as of December 31, 2015, and 1.0 million, 0.8 million, 0.5 million and 1.8 million warrants to purchase additional shares of COCP, ARNO, Sevion and MabVax, respectively. We recorded the changes in the fair value of the options and warrants in Fair value changes of derivative instruments, net in our Consolidated Statements of Operations. We record the fair value of the options and warrants in Investments, net in our Consolidated Balance Sheets. See further discussion of the Company’s options and warrants in Note 17 and Note 18.
Investments in variable interest entities
We have determined that we hold variable interests in Zebra Biologics, Inc. (“Zebra”). We made this determination as a result of our assessment that Zebra does not have sufficient resources to carry out its principal activities without additional financial support.
We own 1,260,000 shares of Zebra Series A-2 Preferred Stock and 900,000 shares of Zebra restricted common stock (ownership 29% at December 31, 2015). Zebra is a privately held biotechnology company focused on the discovery and development of biosuperior antibody therapeutics and complex drugs. Dr. Richard Lerner, M.D., a member of our Board of Directors, is a founder of Zebra and, along with Dr. Frost, serves as a member of Zebra’s Board of Directors.
In order to determine the primary beneficiary of Zebra, we evaluated our investment and our related parties’ investment, as well as our investment combined with the related party group’s investment to identify if we had the power to direct the activities that most significantly impact the economic performance of Zebra. We determined that we do not have the power to direct the activities that most significantly impact Zebra’s economic performance. Based on the capital structure, governing documents and overall business operations of Zebra, we determined that, while a VIE, we do not have the power to direct the activities that most significantly impact Zebra’s economic performance. We did determine, however, that we can significantly influence the success of Zebra through our board representation and voting power. Therefore, we have the ability to exercise significant influence over Zebra’s operations and account for our investment in Zebra under the equity method.
Investment in SciVac
In June 2012, we acquired a 50% stock ownership in SciVac from FDS Pharma LLP (“FDS”). SciVac was a privately-held Israeli company that produced a third-generation hepatitis B-vaccine. From November 2012 through June 2015, we loaned to SciVac a combined $7.9 million for working capital purposes. We determined that we held variable interests in SciVac based on our assessment that SciVac did not have sufficient resources to carry out its principal activities without financial support. We had also determined we were the primary beneficiary of SciVac through our representation on SciVac’s board of directors. SciVac’s board of directors consisted of 5 members, of which 3 members had been appointed by us, representing 60% of SciVac’s board. As a result of this conclusion, we consolidated the results of operations and financial position of SciVac through June 2015 and recorded a reduction of equity for the portion of SciVac we do not own.
On July 9, 2015, SciVac Therapeutics Inc., formerly Levon Resources Ltd. (“STI”) completed a reverse takeover transaction (the “Arrangement”) pursuant to which STI acquired all of the issued and outstanding securities of SciVac. As a result of this transaction, OPKO’s ownership in STI decreased to 24.5%.
92
Upon completion of the Arrangement, we determined that STI was not a VIE. We also determined that we do not have the power to direct the activities that most significantly impact the economic performance of STI that would require us to consolidate STI. STI’s board of directors consists of 7 members, of which 3 independent members are initially members of our management. We do not have any rights to appoint members to STI’s board. STI’s board members are approved by a vote of the shareholders. We recorded a $15.9 million gain on the deconsolidation of SciVac in Other income (expense), net in our Consolidated Statement of Operations for the year ended December 31, 2015. The recognized gain was primarily due to the fair value of the retained interest in STI based on Levon’s cash contribution of approximately $21.2 million under the Arrangement.
Following the deconsolidation, we account for our investment in STI under the equity method as we have determined that we and/or our related parties can significantly influence STI through our board representation and voting power. STI is considered a related party as a result of our board representation in STI and executive management’s ownership interests in STI.
In October 2015, STI announced it entered into an agreement and plan of merger pursuant to which a newly-formed wholly-owned subsidiary of STI will merge with and into VBI Vaccines Inc. (“VBI”) with VBI surviving the merger as a wholly-owned subsidiary of STI, and STI will change its name to VBI Vaccines Inc. At the effective time of the merger, each share of VBI common stock will be converted into the right to receive 20.808356 common shares of STI (the “Exchange Ratio”). Upon closing of the transaction in 2016, holders of VBI’s securities will receive shares, options and warrants of STI representing approximately 46% of the fully diluted outstanding shares of the combined company.
The following table represents the consolidated assets and non-recourse liabilities related to SciVac as of December 31, 2014. These assets were owned by, and these liabilities were obligations of, SciVac, not us.
(In thousands) |
December 31, 2014 |
||
Assets |
|||
Current assets: |
|||
Cash and cash equivalents |
$ |
393 |
|
Accounts receivable, net |
316 |
||
Inventories, net |
1,649 |
||
Prepaid expenses and other current assets |
718 |
||
Total current assets |
3,076 |
||
Property, plant and equipment, net |
1,725 |
||
Intangible assets, net |
875 |
||
Goodwill |
1,553 |
||
Other assets |
384 |
||
Total assets |
$ |
7,613 |
|
Liabilities |
|||
Current liabilities: |
|||
Accounts payable |
$ |
445 |
|
Accrued expenses |
4,446 |
||
Notes payable |
5,189 |
||
Total current liabilities |
10,080 |
||
Other long-term liabilities |
2,042 |
||
Total liabilities |
$ |
12,122 |
|
93
Note 5 Composition of Certain Financial Statement Captions
For the years ended December 31, |
|||||||
(In thousands) |
2015 |
2014 |
|||||
Accounts receivable, net |
|||||||
Accounts receivable |
$ |
219,043 |
$ |
21,875 |
|||
Less: allowance for doubtful accounts |
(25,168 |
) |
(1,906 |
) |
|||
$ |
193,875 |
$ |
19,969 |
||||
Inventories, net |
|||||||
Consumable supplies |
$ |
22,265 |
$ |
— |
|||
Finished products |
13,404 |
12,116 |
|||||
Work in-process |
1,215 |
1,011 |
|||||
Raw materials |
3,848 |
4,116 |
|||||
Less: inventory reserve |
(1,051 |
) |
(639 |
) |
|||
$ |
39,681 |
$ |
16,604 |
||||
Prepaid expenses and other current assets |
|||||||
Other receivables |
$ |
11,946 |
$ |
669 |
|||
Prepaid supplies |
8,773 |
1,123 |
|||||
Taxes recoverable |
3,076 |
2,417 |
|||||
Prepaid insurance |
2,206 |
968 |
|||||
Other |
903 |
4,212 |
|||||
$ |
26,904 |
$ |
9,389 |
||||
Property, plant and equipment, net: |
|||||||
Machinery, medical and other equipment |
$ |
89,936 |
$ |
13,710 |
|||
Leasehold improvements |
27,949 |
3,592 |
|||||
Furniture and fixtures |
11,403 |
2,148 |
|||||
Automobiles and aircraft |
10,271 |
— |
|||||
Software |
10,497 |
1,695 |
|||||
Building |
5,965 |
3,171 |
|||||
Land |
2,394 |
2,391 |
|||||
Construction in process |
425 |
225 |
|||||
Less: accumulated depreciation |
(27,042 |
) |
(10,521 |
) |
|||
$ |
131,798 |
$ |
16,411 |
||||
Intangible assets, net: |
|||||||
Customer relationships |
$ |
449,972 |
$ |
22,108 |
|||
Technologies |
151,709 |
52,508 |
|||||
Trade names |
50,416 |
3,483 |
|||||
Covenants not to compete |
8,612 |
8,639 |
|||||
Licenses |
23,432 |
— |
|||||
Product registrations |
7,512 |
8,763 |
|||||
Other |
5,600 |
1,079 |
|||||
Less: accumulated amortization |
(59,101 |
) |
(33,931 |
) |
|||
$ |
638,152 |
$ |
62,649 |
||||
Accrued expenses: |
|||||||
Deferred revenue |
70,246 |
4,185 |
|||||
Employee benefits |
29,751 |
4,127 |
|||||
Taxes payable |
$ |
7,605 |
$ |
77 |
|||
Contingent consideration |
22,164 |
27,352 |
|||||
94
For the years ended December 31, |
|||||||
Clinical trials |
2,505 |
8,643 |
|||||
Capital leases short-term |
5,373 |
— |
|||||
Milestone payment |
5,000 |
— |
|||||
Professional fees |
1,506 |
1,860 |
|||||
Other |
23,749 |
14,668 |
|||||
$ |
167,899 |
$ |
60,912 |
||||
Other long-term liabilities: |
|||||||
Deferred revenue |
$ |
162,634 |
$ |
2,526 |
|||
JP Morgan Chase line of credit |
72,107 |
— |
|||||
Contingent consideration |
32,258 |
44,215 |
|||||
Capital leases long-term |
9,285 |
— |
|||||
Mortgages and other debts payable |
2,523 |
2,434 |
|||||
Other |
13,663 |
1,030 |
|||||
$ |
292,470 |
$ |
50,205 |
||||
The following table summarizes the fair values assigned to our major intangible asset classes upon each acquisition:
(In thousands) |
Technologies |
In-process research and development |
Customer relationships |
Product registrations |
Covenants not to compete |
Trade names |
Other |
Total identified intangible assets |
Goodwill |
||||||||||||||||||||||||||
Bio-Reference |
$ |
100,600 |
$ |
— |
$ |
395,200 |
$ |
— |
$ |
— |
$ |
47,100 |
$ |
— |
$ |
542,900 |
$ |
441,158 |
|||||||||||||||||
CURNA |
— |
10,000 |
— |
— |
— |
— |
290 |
10,290 |
4,827 |
||||||||||||||||||||||||||
EirGen |
— |
560 |
34,155 |
— |
— |
— |
3,919 |
38,634 |
83,373 |
||||||||||||||||||||||||||
FineTech |
2,700 |
— |
14,200 |
— |
1,500 |
400 |
— |
18,800 |
11,623 |
||||||||||||||||||||||||||
OPKO Biologics |
— |
590,200 |
— |
— |
— |
— |
— |
590,200 |
139,784 |
||||||||||||||||||||||||||
|
OPKO
Chile
|
— |
— |
3,945 |
5,829 |
— |
1,032 |
— |
10,806 |
5,441 |
||||||||||||||||||||||||||
OPKO Diagnostics |
44,400 |
— |
— |
— |
— |
— |
— |
44,400 |
17,977 |
||||||||||||||||||||||||||
OPKO Health Europe |
3,017 |
1,459 |
436 |
2,930 |
187 |
349 |
— |
8,378 |
8,062 |
||||||||||||||||||||||||||
OPKO Lab |
1,370 |
— |
3,860 |
— |
6,900 |
1,830 |
70 |
14,030 |
29,629 |
||||||||||||||||||||||||||
OPKO Renal |
— |
191,530 |
— |
— |
— |
— |
210 |
191,740 |
2,411 |
||||||||||||||||||||||||||
Weighted average amortization period |
8-12 years |
Indefinite |
6-20 years |
9 years |
5 years |
4-5 years |
3-10 years |
Indefinite |
|||||||||||||||||||||||||||
All of the intangible assets and goodwill acquired relate to our acquisitions of principally OPKO Renal, OPKO Biologics, EirGen and Bio-Reference. We do not anticipate capitalizing the cost of product registration renewals, rather we expect to expense these costs, as incurred. Our goodwill is not tax deductible for income tax purposes in any jurisdiction we operate in.
At December 31, 2015, the changes in value of the intangible assets and goodwill are primarily due to the acquisitions of Bio-Reference and EirGen and foreign currency fluctuations between the Chilean and Mexican pesos, the Euro and the Shekel against the U.S. dollar. At December 31, 2014, the changes in value of the intangible assets and goodwill are primarily due to foreign currency fluctuations between the Chilean and Mexican pesos, the Euro and the Shekel against the U.S. dollar.
The following table reflects the changes in the allowance for doubtful accounts, provision for inventory reserve and tax valuation allowance accounts:
95
(In thousands) |
Beginning
balance
|
Charged
to
expense
|
Written-off |
Charged
to other
|
Ending
balance
|
|||||||||||
2015 |
||||||||||||||||
Allowance for doubtful accounts |
$ |
(1,906 |
) |
(24,548 |
) |
928 |
358 |
$ |
(25,168 |
) |
||||||
Inventory reserve |
$ |
(639 |
) |
(926 |
) |
435 |
79 |
$ |
(1,051 |
) |
||||||
Tax valuation allowance |
$ |
(131,931 |
) |
— |
— |
89,784 |
$ |
(42,147 |
) |
|||||||
2014 |
||||||||||||||||
Allowance for doubtful accounts |
$ |
(1,884 |
) |
(646 |
) |
321 |
303 |
$ |
(1,906 |
) |
||||||
Inventory reserve |
$ |
(777 |
) |
(1,082 |
) |
1,028 |
192 |
$ |
(639 |
) |
||||||
Tax valuation allowance |
$ |
(85,370 |
) |
— |
— |
(46,561 |
) |
$ |
(131,931 |
) |
||||||
The following table summarizes the changes in Goodwill during the year ended December 31, 2015.
2015 |
2014 |
||||||||||||||||||||||||||||||
(In thousands) |
Balance at January 1st |
Acquisitions |
Foreign exchange, other |
Balance at December 31st |
Balance at January 1 |
Acquisitions |
Foreign exchange, other |
Balance at December 31 |
|||||||||||||||||||||||
Pharmaceuticals |
|||||||||||||||||||||||||||||||
CURNA |
$ |
4,827 |
$ |
— |
$ |
— |
$ |
4,827 |
$ |
4,827 |
$ |
— |
$ |
— |
$ |
4,827 |
|||||||||||||||
EirGen |
— |
83,373 |
(2,234 |
) |
81,139 |
— |
— |
— |
— |
||||||||||||||||||||||
FineTech |
11,698 |
— |
— |
11,698 |
11,698 |
— |
— |
11,698 |
|||||||||||||||||||||||
OPKO Biologics |
139,784 |
— |
— |
139,784 |
139,784 |
— |
— |
139,784 |
|||||||||||||||||||||||
OPKO Chile |
5,283 |
— |
(766 |
) |
4,517 |
6,102 |
— |
(819 |
) |
5,283 |
|||||||||||||||||||||
OPKO Health Europe |
8,013 |
— |
(822 |
) |
7,191 |
9,075 |
— |
(1,062 |
) |
8,013 |
|||||||||||||||||||||
OPKO Mexico |
100 |
— |
(100 |
) |
— |
114 |
— |
(14 |
) |
100 |
|||||||||||||||||||||
OPKO Renal |
2,069 |
— |
— |
2,069 |
2,069 |
— |
— |
2,069 |
|||||||||||||||||||||||
SciVac |
1,553 |
— |
(1,553 |
) |
— |
1,739 |
— |
(186 |
) |
1,553 |
|||||||||||||||||||||
Diagnostics |
|||||||||||||||||||||||||||||||
Bio-Reference |
— |
441,158 |
— |
441,158 |
— |
— |
— |
— |
|||||||||||||||||||||||
OPKO Diagnostics |
17,977 |
— |
— |
17,977 |
17,977 |
— |
— |
17,977 |
|||||||||||||||||||||||
OPKO Lab |
32,988 |
— |
— |
32,988 |
32,988 |
— |
— |
32,988 |
|||||||||||||||||||||||
$ |
224,292 |
$ |
524,531 |
$ |
(5,475 |
) |
$ |
743,348 |
$ |
226,373 |
$ |
— |
$ |
(2,081 |
) |
$ |
224,292 |
||||||||||||||
96
Note 6 Debt
In January 2013, we entered into note purchase agreements (the “2033 Senior Notes”) with qualified institutional buyers and accredited investors (collectively, the “Purchaser”) in a private placement in reliance on exemptions from registration under the Securities Act of 1933, (the “Securities Act”). The Purchasers of the 2033 Senior Notes include Frost Gamma Investments Trust, a trust affiliated with Dr. Frost, and Hsu Gamma Investment, L.P., an entity affiliated with Dr. Jane H. Hsiao, our Vice Chairman and Chief Technology Officer. The 2033 Senior Notes were issued on January 30, 2013. The 2033 Senior Notes, which totaled $175.0 million, bear interest at the rate of 3.00% per year, payable semiannually on February 1 and August 1 of each year, beginning August 1, 2013. The 2033 Senior Notes will mature on February 1, 2033, unless earlier repurchased, redeemed or converted. Upon a fundamental change as defined in the instruments governing the 2033 Senior Notes, subject to certain exceptions, the holders may require us to repurchase all or any portion of their 2033 Senior Notes for cash at a repurchase price equal to 100% of the principal amount of the 2033 Senior Notes being repurchased, plus any accrued and unpaid interest to but not including the fundamental change repurchase date.
The following table sets forth information related to the 2033 Senior Notes which is included our Consolidated Balance Sheets as of December 31, 2015:
(In thousands) |
Embedded conversion option |
2033 Senior Notes |
Discount |
Total |
|||||||||||
Balance at December 31, 2014 |
$ |
65,947 |
$ |
87,642 |
$ |
(22,135 |
) |
$ |
131,454 |
||||||
Amortization of debt discount |
— |
— |
2,613 |
2,613 |
|||||||||||
Change in fair value of embedded derivative |
36,587 |
— |
— |
36,587 |
|||||||||||
Conversion |
(78,797 |
) |
(55,442 |
) |
12,997 |
(121,242 |
) |
||||||||
Balance at December 31, 2015 |
$ |
23,737 |
$ |
32,200 |
$ |
(6,525 |
) |
$ |
49,412 |
||||||
The following table sets forth information related to the 2033 Senior Notes which is included our Consolidated Balance Sheets as of December 31, 2014:
(In thousands) |
Embedded conversion option |
2033 Senior Notes |
Discount |
Total |
|||||||||||
Balance at December 31, 2013 |
$ |
101,087 |
$ |
158,064 |
$ |
(47,239 |
) |
$ |
211,912 |
||||||
Amortization of debt discount |
— |
— |
5,662 |
5,662 |
|||||||||||
Change in fair value of embedded derivative |
12,213 |
— |
— |
12,213 |
|||||||||||
Conversion |
(47,353 |
) |
(70,422 |
) |
19,442 |
(98,333 |
) |
||||||||
Balance at December 31, 2014 |
$ |
65,947 |
$ |
87,642 |
$ |
(22,135 |
) |
$ |
131,454 |
||||||
The 2033 Senior Notes will be convertible at any time on or after November 1, 2032, through the second scheduled trading day immediately preceding the maturity date, at the option of the holders. Additionally, holders may convert their 2033 Senior Notes prior to the close of business on the scheduled trading day immediately preceding November 1, 2032, under the following circumstances: (1) conversion based upon satisfaction of the trading price condition relating to the 2033 Senior Notes; (2) conversion based on the Common Stock price; (3) conversion based upon the occurrence of specified corporate events; or (4) if we call the 2033 Senior Notes for redemption. The 2033 Senior Notes will be convertible into cash, shares of our Common Stock, or a combination of cash and shares of Common Stock, at our election unless we have made an irrevocable election of net share settlement. The initial conversion rate for the 2033 Senior Notes will be 141.48 shares of Common Stock per $1,000 principal amount of 2033 Senior Notes (equivalent to an initial conversion price of approximately $7.07 per share of Common Stock), and will be subject to adjustment upon the occurrence of certain events. In addition, we will, in certain circumstances, increase the conversion rate for holders who convert their 2033 Senior Notes in connection with a make-whole fundamental change (as defined in the Indenture) and holders who convert upon the occurrence of certain specific events prior to February 1, 2017 (other than in connection with a make-whole fundamental change). Holders of the 2033 Senior Notes may require us to repurchase the 2033 Senior Notes for 100% of their principal amount, plus accrued and unpaid interest, on February 1, 2019, February 1, 2023 and February 1, 2028, or following the occurrence of a fundamental change as defined in the indenture governing the 2033 Senior Notes. See further discussion in Note 20.
We may not redeem the 2033 Senior Notes prior to February 1, 2017. On or after February 1, 2017 and before February 1, 2019, we may redeem for cash any or all of the 2033 Senior Notes but only if the last reported sale price of our Common Stock exceeds 130% of the applicable conversion price for at least 20 trading days during the 30 consecutive trading day period ending on the trading day immediately prior to the date on which we deliver the redemption notice. The redemption
97
price will equal 100% of the principal amount of the 2033 Senior Notes to be redeemed, plus any accrued and unpaid interest to but not including the redemption date. On or after February 1, 2019, we may redeem for cash any or all of the 2033 Senior Notes at a redemption price of 100% of the principal amount of the 2033 Senior Notes to be redeemed, plus any accrued and unpaid interest up to but not including the redemption date.
The terms of the 2033 Senior Notes, include, among others: (i) rights to convert into shares of our Common Stock, including upon a fundamental change; and (ii) a coupon make-whole payment in the event of a conversion by the holders of the 2033 Senior Notes on or after February 1, 2017 but prior to February 1, 2019. We have determined that these specific terms are considered to be embedded derivatives. Embedded derivatives are required to be separated from the host contract, the 2033 Senior Notes, and carried at fair value when: (a) the embedded derivative possesses economic characteristics that are not clearly and closely related to the economic characteristics of the host contract; and (b) a separate, stand-alone instrument with the same terms would qualify as a derivative instrument. We have concluded that the embedded derivatives within the 2033 Senior Notes meet these criteria and, as such, must be valued separate and apart from the 2033 Senior Notes and recorded at fair value each reporting period.
For accounting and financial reporting purposes, we combine these embedded derivatives and value them together as one unit of accounting. At each reporting period, we record these embedded derivatives at fair value which is included as a component of the 2033 Senior Notes on our Consolidated Balance Sheets.
On August 30, 2013, one of the conversion rights in the 2033 Senior Notes was triggered. Holders of the 2033 Senior Notes converted $16.9 million principal amount into 2,396,145 shares of our Common Stock at a rate of 141.48 shares of Common Stock per $1,000 principal amount of 2033 Senior Notes. We recorded a $1.0 million non-cash gain related to the conversion. The gain on exchange is included within Other income (expense) on our Consolidated Statement of Operations.
In June 2014, we entered into an exchange agreement with a holder of the Company’s 2033 Senior Notes pursuant to which such holder exchanged $70.4 million in aggregate principal amount of Notes for 10,974,431 shares of the Company’s Common Stock and approximately $0.8 million in cash representing accrued interest through the date of completion of the exchange. We recorded a $2.7 million non-cash gain related to the exchange.
On April 1, 2015, we announced that our 2033 Senior Notes are convertible by holders of such notes. We have elected to satisfy our conversion obligation under the 2033 Senior Notes in shares of our Common Stock. This conversion right was triggered because the closing price per share of our Common Stock has exceeded $9.19, or 130% of the initial conversion price of $7.07, for at least 3 of 30 consecutive trading days during the period ending on March 31, 2015. The 2033 Senior Notes were convertible until June 30, 2015, and may be convertible thereafter, if one or more of the conversion conditions specified in the Indenture, dated as of January 30, 2013, by and between the Company and Wells Fargo Bank N.A., is satisfied during future measurement periods. Pursuant to the Indenture, a holder who elects to convert the 2033 Senior Notes will receive 141.4827 shares of our Common Stock plus such number of additional shares as is applicable on the conversion date per $1,000 principal amount of 2033 Senior Notes based on the early conversion provisions in the Indenture. On July 1, 2015, October 1, 2015 and January 5, 2016, we announced that our 2033 Senior Notes continue to be convertible by holders of such notes during the third quarter of 2015, the fourth quarter of 2015 and the first quarter of 2016, respectively.
During 2015, pursuant to the conversion right or through exchange agreements we entered with certain holders of our 2033 Senior Notes, holders of our 2033 Senior Notes converted or exchanged $55.4 million in aggregate principal amount of 2033 Senior Notes for 8,118,062 shares of the Company’s Common Stock. We recorded a $0.9 million non-cash gain related to the conversion and exchanges. The gain is included within Other income (expense) in our Consolidated Statement of Operations.
We used a binomial lattice model in order to estimate the fair value of the embedded derivative in the 2033 Senior Notes. A binomial lattice model generates two probable outcomes — one up and another down —arising at each point in time, starting from the date of valuation until the maturity date. A lattice model was initially used to determine if the 2033 Senior Notes would be converted, called or held at each decision point. Within the lattice model, the following assumptions are made: (i) the 2033 Senior Notes will be converted early if the conversion value is greater than the holding value; or (ii) the 2033 Senior Notes will be called if the holding value is greater than both (a) the redemption price (as defined in the Indenture) and (b) the conversion value plus the coupon make-whole payment at the time. If the 2033 Senior Notes are called, then the holder will maximize their value by finding the optimal decision between (1) redeeming at the redemption price and (2) converting the 2033 Senior Notes.
Using this lattice model, we valued the embedded derivatives using the “with-and-without method,” where the value of the 2033 Senior Notes including the embedded derivatives is defined as the “with,” and the value of the 2033 Senior Notes excluding the embedded derivatives is defined as the “without.” This method estimates the value of the embedded derivatives
98
by looking at the difference in the values between the 2033 Senior Notes with the embedded derivatives and the value of the 2033 Senior Notes without the embedded derivatives.
The lattice model requires the following inputs: (i) price of our Common Stock; (ii) Conversion Rate (as defined in the Indenture); (iii) Conversion Price (as defined in the Indenture); (iv) maturity date; (v) risk-free interest rate; (vi) estimated stock volatility; and (vii) estimated credit spread for the Company.
The following table sets forth the inputs to the lattice model used to value the embedded derivative:
December 31, 2015 |
December 31, 2014 |
December 31, 2013 |
|||
Stock price |
$10.05 |
$9.99 |
$8.44 |
||
Conversion Rate |
141.4827 |
141.4827 |
141.4827 |
||
Conversion Price |
$7.07 |
$7.07 |
$7.07 |
||
Maturity date |
February 1, 2033 |
February 1, 2033 |
February 1, 2033 |
||
Risk-free interest rate |
1.33% |
1.40% |
1.78% |
||
Estimated stock volatility |
50% |
39% |
55% |
||
Estimated credit spread |
1,142 basis points |
1,081 basis points |
828 basis points |
||
The following table sets forth the fair value of the 2033 Senior Notes with and without the embedded derivatives, and the fair value of the embedded derivatives at December 31, 2015, 2014 and 2013. At December 31, 2015, 2014 and 2013, the principal amount of the 2033 Senior Notes was $32.2 million, $87.6 million and $158.1 million, respectively:
(In thousands) |
December 31, 2015 |
December 31, 2014 |
December 31, 2013 |
||||||||
Fair value of 2033 Senior Notes: |
|||||||||||
With the embedded derivatives |
$ |
48,384 |
$ |
129,009 |
$ |
218,081 |
|||||
Without the embedded derivatives |
$ |
24,647 |
$ |
63,062 |
$ |
116,994 |
|||||
Estimated fair value of the embedded derivatives |
$ |
23,737 |
$ |
65,947 |
$ |
101,087 |
|||||
Changes in certain inputs into the lattice model can have a significant impact on changes in the estimated fair value of the embedded derivatives. For example, a decrease in our estimated credit spread results in an increase in the estimated value of the embedded derivatives. Conversely, a decrease in the price of our Common Stock results in a decrease in the estimated fair value of the embedded derivatives. For the years ended December 31, 2015 and 2014, we observed an increase in the market price of our Common Stock which primarily resulted in a $36.6 million and $12.2 million increase, respectively, in the estimated fair value of our embedded derivatives recorded in Fair value changes of derivative instruments, net in our Consolidated Statements of Operations.
On November 5, 2015, Bio-Reference and certain of its subsidiaries entered into a credit agreement with JPMorgan Chase Bank, N.A. (“CB”), as lender and administrative agent (the “Credit Agreement”), which replaced Bio-Reference’s existing credit facility with PNC Bank, National Association (“PNC”). The Credit Agreement provides for a $175.0 million secured revolving credit facility and includes a $20.0 million sub-facility for swingline loans and a $20.0 million sub-facility for the issuance of letters of credit. Bio-Reference may increase the credit facility to up to $275.0 million on a secured basis, subject to the satisfaction of specified conditions. The Credit Agreement matures on November 5, 2020 and is guaranteed by all of Bio-Reference’s domestic subsidiaries. The Credit Agreement is also secured by substantially all assets of Bio-Reference and its domestic subsidiaries, as well as a non-recourse pledge by us of our equity interest in Bio-Reference. Availability under the Credit Agreement is based on a borrowing base comprised of eligible accounts receivables of Bio-Reference and certain of its subsidiaries, as specified therein. The proceeds of the new credit facility were used to refinance existing indebtedness, including amounts outstanding under the credit facility with PNC which was terminated in 2015 in accordance with its terms, to finance working capital needs and for general corporate purposes of Bio-Reference and its subsidiaries.
At Bio-Reference’s option, borrowings under the Credit Agreement (other than swingline loans) will bear interest at (i) the CB floating rate (defined as the higher of (a) the prime rate and (b) the LIBOR rate (adjusted for statutory reserve requirements for Eurocurrency liabilities) for an interest period of one month plus 2.50%) plus an applicable margin of 0.35% for the first 12 months and 0.50% thereafter or (ii) the LIBOR rate (adjusted for statutory reserve requirements for Eurocurrency liabilities) plus an applicable margin of 1.35% for the first 12 months and 1.50% thereafter. Swingline loans will bear interest at the CB floating rate plus the applicable margin. The Credit Agreement also calls for other customary fees and charges, including an unused commitment fee of 0.25% of the lending commitments.
99
The Credit Agreement contains customary covenants and restrictions, including, without limitation, covenants that require Bio-Reference and its subsidiaries to maintain a minimum fixed charge coverage ratio if availability under the new credit facility falls below a specified amount and to comply with laws, and restrictions on the ability of Bio-Reference and its subsidiaries to incur additional indebtedness or to pay dividends and make certain other distributions to the Company, subject to certain exceptions as specified therein. Failure to comply with these covenants would constitute an event of default under the Credit Agreement, notwithstanding the ability of Bio-Reference to meet its debt service obligations. The Credit Agreement also includes various customary remedies for the lenders following an event of default, including the acceleration of repayment of outstanding amounts under the Credit Agreement and execution upon the collateral securing obligations under the Credit Agreement. Substantially all the assets of Bio-Reference and its subsidiaries are restricted from sale, transfer, lease, disposal or distributions to the Company, subject to certain exceptions. Bio-Reference and its subsidiaries net assets as of December 31, 2015 was approximately $1.0 billion, which includes goodwill of $441.2 million and intangible assets of $528.3 million.
We have line of credit agreements with ten financial institutions as of December 31, 2015 and ten financial institutions as of December 31, 2014 in United States, Chile and Spain. These lines of credit are used primarily as a source of working capital for inventory purchases.
The following table summarizes the amounts outstanding under the Bio-Reference, Chilean and Spanish lines of credit:
(Dollars in thousands) |
Balance Outstanding |
|||||||||||||
Lender |
Interest rate on
borrowings at December 31, 2015
|
Credit line
capacity
|
December 31, 2015 |
December 31,
2014
|
||||||||||
JP Morgan Chase |
3.25% |
$ |
175,000 |
$ |
72,107 |
$ |
— |
|||||||
Itau Bank |
6.00% |
1,500 |
282 |
965 |
||||||||||
Bank of Chile |
5.50% |
2,500 |
2,313 |
1,410 |
||||||||||
BICE Bank |
5.50% |
2,300 |
1,502 |
1,249 |
||||||||||
BBVA Bank |
5.50% |
2,300 |
1,825 |
795 |
||||||||||
Penta Bank |
7.58% |
— |
— |
1,008 |
||||||||||
Security Bank |
6.16% |
150 |
145 |
361 |
||||||||||
Estado Bank |
5.30% |
2,500 |
2,210 |
1,870 |
||||||||||
Santander Bank |
5.30% |
2,000 |
1,345 |
— |
||||||||||
Scotiabank |
5.00% |
1,300 |
939 |
— |
||||||||||
Banco Bilbao Vizcaya |
2.90% |
273 |
— |
— |
||||||||||
Total |
$ |
189,823 |
$ |
82,668 |
$ |
7,658 |
||||||||
At December 31, 2015 and 2014, the weighted average interest rate on our lines of credit was approximately 4.3% and 6.1%, respectively.
At December 31, 2015 and 2014, we had mortgage notes and other debt (excluding the 2033 Senior Notes, the Credit Agreement and amounts outstanding under lines of credit) as follows:
(In thousands) |
December 31, 2015 |
December 31,
2014
|
|||||
Current portion of notes payable |
$ |
1,054 |
$ |
608 |
|||
Other long-term liabilities |
1,963 |
2,435 |
|||||
Total mortgage notes and other debt |
$ |
3,017 |
$ |
3,043 |
|||
The mortgages and other debts mature at various dates ranging from 2015 through 2024 bearing variable interest rates from 2.4% up to 6.3%. The weighted average interest rate on the mortgage notes and other debt at December 31, 2015 and 2014, was 4.3% and 3.4%, respectively. The mortgages are secured by our office space in Barcelona.
100
Note 7 Shareholders’ Equity
Our authorized capital stock consists of 750,000,000 shares of Common Stock, par value $0.01 per share, and 10,000,000 shares of Preferred Stock, par value $0.01 per share.
Common Stock
Subject to the rights of the holders of any shares of Preferred Stock currently outstanding or which may be issued in the future, the holders of the Common Stock are entitled to receive dividends from our funds legally available when, as and if declared by our Board of Directors, and are entitled to share ratably in all of our assets available for distribution to holders of Common Stock upon the liquidation, dissolution or winding-up of our affairs subject to the liquidation preference, if any, of any then outstanding shares of Preferred Stock. Holders of our Common Stock do not have any preemptive, subscription, redemption or conversion rights. Holders of our Common Stock are entitled to one vote per share on all matters which they are entitled to vote upon at meetings of stockholders or upon actions taken by written consent pursuant to Delaware corporate law. The holders of our Common Stock do not have cumulative voting rights, which means that the holders of a plurality of the outstanding shares can elect all of our directors. All of the shares of our Common Stock currently issued and outstanding are fully-paid and nonassessable. No dividends have been paid to holders of our Common Stock since our incorporation, and no cash dividends are anticipated to be declared or paid on our Common Stock in the reasonably foreseeable future.
In addition to our equity-based compensation plans, we have issued warrants to purchase our Common Stock. Refer to Note 9 for additional information on our share-based compensation plans. The table below provides additional information for warrants outstanding as of December 31, 2015.
Warrants |
Number of
warrants
|
Weighted
average
exercise price
|
Expiration date |
||||||
Outstanding at December 31, 2014 |
* |
21,239,213 |
$ |
0.75 |
Various from July 2015 through March 2017 |
||||
Exercised |
(19,034,662 |
) |
0.74 |
||||||
Expired |
(30,828 |
) |
0.01 |
||||||
Outstanding and Exercisable at December 31, 2015 |
2,173,723 |
$ |
0.85 |
Various from January 2017 through March 2017 |
|||||
* Prior year reported amounts adjusted by 190,533 warrants that expired in September 2014.
Of the 19,034,662 Common Stock warrants exercised, 1,197,932 shares were surrendered in lieu of a cash payment via the net exercise feature of the warrant agreements.
Preferred Stock
Under our certificate of incorporation, our Board of Directors has the authority, without further action by stockholders, to designate up to 10 million shares of Preferred Stock in one or more series and to fix or alter, from time to time, the designations, powers and rights of each series of Preferred Stock and the qualifications, limitations or restrictions of any series of Preferred Stock, including dividend rights, dividend rate, conversion rights, voting rights, rights and terms of redemption (including sinking fund provisions), redemption price or prices, and the liquidation preference of any wholly issued series of Preferred Stock, any or all of which may be greater than the rights of the Common Stock, and to establish the number of shares constituting any such series.
Of the authorized Preferred Stock, 4,000,000 shares, 500,000 shares and 2,000,000 shares were designated Series A Preferred Stock, Series C Preferred Stock and Series D Preferred Stock, respectively. As of December 31, 2015 and 2014, there were no shares of Series A Preferred Stock, Series C Preferred Stock or Series D Preferred Stock issued or outstanding.
101
Note 8 Accumulated Other Comprehensive Income (Loss)
For the year ended December 31, 2015, changes in Accumulated other comprehensive income (loss), net of tax, were as follows:
(In thousands) |
Foreign currency translation |
Unrealized
gain (loss) in
Accumulated
OCI
|
Total |
||||||||
Balance at December 31, 2014 |
$ |
(6,717 |
) |
$ |
(5,675 |
) |
$ |
(12,392 |
) |
||
Other comprehensive income (loss) before reclassifications, net of tax (1)
|
(15,074 |
) |
(2,378 |
) |
(17,452 |
) |
|||||
Amounts reclassified from accumulated other comprehensive income (loss), net of tax (1)
|
— |
7,307 |
7,307 |
||||||||
Net other comprehensive loss |
(15,074 |
) |
4,929 |
(10,145 |
) |
||||||
Balance at December 31, 2015 |
$ |
(21,791 |
) |
$ |
(746 |
) |
$ |
(22,537 |
) |
||
(1) |
Effective tax rate of 40.13%.
|
Amounts reclassified from Accumulated other comprehensive income (loss) for the year ended December 31, 2015 includes an other-than-temporary impairment charge on our investment in RXi as discussed in Note 4. Amounts reclassified for our available for sale investments were based on the specific identification method.
For the year ended December 31, 2014, changes in Accumulated other comprehensive income, net of tax, were as follows:
(In thousands) |
Foreign currency translation |
Unrealized gain (loss) in Accumulated OCI |
Total |
||||||||
Balance at December 31, 2013 |
$ |
1,371 |
$ |
2,047 |
$ |
3,418 |
|||||
Other comprehensive income (loss) before reclassifications, net of tax (1)
|
(8,088 |
) |
(8,044 |
) |
(16,132 |
) |
|||||
Amounts reclassified from accumulated other comprehensive income, net of tax (1)
|
— |
322 |
322 |
||||||||
Net other comprehensive loss |
(8,088 |
) |
(7,722 |
) |
(15,810 |
) |
|||||
Balance at December 31, 2014 |
$ |
(6,717 |
) |
$ |
(5,675 |
) |
$ |
(12,392 |
) |
||
(1) |
Effective tax rate of 40.13%.
|
Amounts reclassified from Accumulated other comprehensive income (loss) for the year ended December 31, 2014, includes $1.3 million realized gain on the sales of certain of our investments available for sale. Of the $1.3 million gain on the sales of our investments available for sale, a $0.9 million gain was reclassified from unrealized gains in Accumulated other comprehensive income (loss) to Other income (expense), net for the year ended December 31, 2014. Amounts reclassified from Accumulated other comprehensive income (loss) also includes an other-than-temporary impairment charge on our investment in ARNO as discussed in Note 4. Amounts reclassified for our available for sale investments were based on the specific identification method.
102
Note 9 Equity-Based Compensation
We maintain five equity-based incentive compensation plans, the Acuity Pharmaceuticals, Inc. 2003 Equity Incentive Plan, the 2007 Equity Incentive Plan, the 2000 Stock Option Plan, the Bio-Reference Laboratories, Inc. 2003 Employee Incentive Stock Option Plan, the Modigene Inc. 2005 Stock Incentive Plan and the Modigene Inc. 2007 Equity Incentive Plan that provide for grants of stock options and restricted stock to our directors, officers, key employees and certain outside consultants. Equity awards granted under our 2007 Equity Incentive Plan are exercisable for a period of either 7 years or 10 years from the date of grant. Equity awards granted under our 2000 Stock Option Plan, 2003 Equity Incentive Plan and the two Modigene Plans are exercisable for a period of up to 10 years from date of grant. Vesting periods range from immediate to 5 years.
We classify the cash flows resulting from the tax benefit that arises when the tax deductions exceed the compensation cost recognized for those equity awards (excess tax benefits) as financing cash inflows. There were no excess tax benefits for the years ended December 31, 2015, 2014, and 2013.
Equity-based compensation arrangements to non-employees are accounted for at their fair value on the measurement date. The measurement of equity-based compensation to non-employees is subject to periodic adjustment over the vesting period of the equity instruments.
Valuation and Expense Information
We recorded equity-based compensation expense of $26.1 million, $14.8 million and $11.0 million for the years ended December 31, 2015, 2014, and 2013, respectively, all of which were reflected as operating expenses. Of the $26.1 million of equity based compensation expense recorded in the year ended December 31, 2015, $17.4 million was recorded as selling, general and administrative expenses, $7.9 million was recorded as research and development expenses and $0.8 million was recorded as a cost of revenue. Of the $14.8 million of equity based compensation expense recorded in the year ended December 31, 2014, $9.7 million was recorded as selling, general and administrative expense and $5.0 million was recorded as research and development expenses and $0.1 million was recorded as a cost of revenue. Of the $11.0 million of equity based compensation expense recorded in the year ended December 31, 2013, $7.3 million was recorded as selling, general and administrative expense and $3.6 million was recorded as research and development expenses.
We estimate forfeitures of stock options and recognize compensation cost only for those awards expected to vest. Forfeiture rates are determined for all employees and non-employee directors based on historical experience and our estimate of future vesting. Estimated forfeiture rates are adjusted from time to time based on actual forfeiture experience.
As of December 31, 2015, there was $90.8 million of unrecognized compensation cost related to the stock options granted under our equity-based incentive compensation plans. Such cost is expected to be recognized over a weighted-average period of approximately 3.0 years.
Stock Options
We estimate the fair value of each stock option on the date of grant using the Black-Scholes-Merton Model option-pricing formula and amortize the fair value to expense over the stock option’s vesting period using the straight-line attribution approach for employees and non-employee directors, and for awards issued to non-employees we recognize compensation expense on a graded basis, with most of the compensation expense being recorded during the initial periods of vesting. We apply the following assumptions in our Black-Scholes-Merton Model option-pricing formula:
|
Year Ended
December 31,
2015
|
Year Ended
December 31,
2014
|
Year Ended
December 31,
2013
|
|||
Expected term (in years) |
1.0 - 10.0 |
1.0 - 10.0 |
1.0 - 7.0 |
||
Risk-free interest rate |
0.26% - 2.42% |
0.10% - 2.65% |
0.15% - 2.45% |
||
Expected volatility |
'32% - 64% |
'31% - 72% |
'31% - 83% |
||
Expected dividend yield |
0% |
0% |
0% |
||
Expected Term: The expected term of the stock options granted to employees and non-employee directors was calculated using the shortcut method. We believe this method is appropriate as our equity shares have been publicly-traded for a limited period of time and as such we do not have sufficient historical exercise data to provide a reasonable basis upon which to estimate expected term. The expected term of stock options issued to non-employee consultants is the remaining contractual life of the options issued.
103
Risk-Free Interest Rate: The risk-free interest rate is based on the rates paid on securities issued by the U.S. Treasury with a term approximating the expected life of the option.
Expected Volatility: The expected volatility for stock options with an expected life of 8 years or less was based on the historical volatility of our stock. The expected volatility for stock options with an expected life of 9 years or greater was based on an average of the volatility of a peer group of publicly-traded entities and the historical volatility of our stock, which we believe will be representative of the volatility over the expected term of the options. We believe the use of peer group’s historical volatility is appropriate as our equity shares have not been publicly-traded for 9 years.
Expected Dividend Yield: We do not intend to pay dividends on Common Stock for the foreseeable future. Accordingly, we used a dividend yield of zero in the assumptions.
We maintain incentive stock plans that provide for the grants of stock options to our directors, officers, employees and non-employee consultants. As of December 31, 2015, there were 2,056,783 shares of Common Stock reserved for issuance under our 2007 Incentive Plan. We intend to issue new shares upon the exercise of stock options. Stock options granted under these plans have been granted at an option price equal to the closing market value of the stock on the date of the grant. Stock options granted under these plans to employees typically become exercisable over four years in equal annual installments after the date of grant, and stock options granted to non-employee directors become exercisable in full one-year after the grant date, subject to, in each case, continuous service with us during the applicable vesting period. We assumed stock options to grant Common Stock as part of the mergers with Acuity Pharmaceuticals, Inc., Froptix, Inc., OPKO Biologics and Bio-Reference, which reflected various vesting schedules, including monthly vesting to employees and non-employee consultants.
A summary of option activity under our stock option plans as of December 31, 2015, and the changes during the year is presented below:
Options |
Number of
options
|
Weighted
average
exercise
price
|
Weighted
average
remaining
contractual
term (years)
|
Aggregate
intrinsic value
(in thousands)
|
||||||||
Outstanding at December 31, 2014 |
23,299,919 |
$ |
5.50 |
5.4 |
$ |
104,797 |
||||||
Granted |
15,579,500 |
$ |
13.09 |
|||||||||
Exercised |
(6,643,991 |
) |
$ |
3.93 |
||||||||
Forfeited |
(710,250 |
) |
$ |
9.64 |
||||||||
Expired |
(238,391 |
) |
$ |
1.58 |
||||||||
Outstanding at December 31, 2015 |
31,286,787 |
$ |
9.55 |
6.97 |
$ |
63,902 |
||||||
Vested and expected to vest at December 31, 2015 |
28,066,315 |
$ |
9.35 |
6.82 |
$ |
60,780 |
||||||
Exercisable at December 31, 2015 |
8,779,201 |
$ |
3.76 |
3.76 |
$ |
41,891 |
||||||
The total intrinsic value of stock options exercised for the years ended December 31, 2015, 2014, and 2013 was $69.9 million, $14.6 million and $59.5 million, respectively.
The weighted average grant date fair value of stock options granted for the years ended December 31, 2015, 2014, and 2013 was $5.00, $4.64, and $4, respectively. The total fair value of stock options vested during the years ended December 31, 2015, 2014, and 2013 was $13.3 million, $10.9 million and $5.9 million, respectively.
Restricted Stock
In 2009, we issued 30,000 shares of restricted Common Stock to one of our independent board members. The restricted stock was granted under our 2007 Equity Incentive Plan with a term of 7 years and vesting occurring 5 years after the grant date with certain events which would accelerate the vesting of the award. The restricted stock was valued using the grant date fair value which was equivalent to the closing price of our Common Stock on the grant date. We record the cost of restricted stock over the vesting period.
104
Note 10 Income Taxes
We operate and are required to file tax returns in the U.S. and various foreign jurisdictions.
The benefit (provision) for incomes taxes consists of the following:
For the years ended December 31, |
|||||||||||
(In thousands) |
2015 |
2014 |
2013 |
||||||||
Current |
|||||||||||
Federal |
$ |
430 |
$ |
225 |
$ |
— |
|||||
State |
(2,157 |
) |
247 |
— |
|||||||
Foreign |
(8,134 |
) |
(1,514 |
) |
(1,073 |
) |
|||||
(9,861 |
) |
(1,042 |
) |
(1,073 |
) |
||||||
Deferred |
|||||||||||
Federal |
109,286 |
— |
(1,161 |
) |
|||||||
State |
12,327 |
(167 |
) |
(104 |
) |
||||||
Foreign |
1,923 |
1,185 |
666 |
||||||||
123,536 |
1,018 |
(599 |
) |
||||||||
Total, net |
$ |
113,675 |
$ |
(24 |
) |
$ |
(1,672 |
) |
|||
Deferred income tax assets and liabilities as of December 31, 2015 and 2014 are comprised of the following:
(In thousands) |
December 31, 2015 |
December 31, 2014 |
|||||
Deferred income tax assets: |
|||||||
Federal net operating loss |
$ |
71,658 |
$ |
63,004 |
|||
State net operating loss |
14,227 |
12,050 |
|||||
Foreign net operating loss |
33,701 |
25,825 |
|||||
Research and development expense |
5,138 |
9,244 |
|||||
Research and development tax credit |
7,388 |
6,077 |
|||||
Stock options |
24,756 |
18,422 |
|||||
Accruals |
7,086 |
1,764 |
|||||
Equity investments |
4,420 |
8,038 |
|||||
Bad debts |
38,809 |
— |
|||||
Lease liability |
7,022 |
— |
|||||
Other |
7,104 |
4,702 |
|||||
Deferred income tax assets |
221,309 |
149,126 |
|||||
Deferred income tax liabilities: |
|||||||
Intangible assets |
(386,588 |
) |
(177,074 |
) |
|||
Fixed assets |
(17,072 |
) |
— |
||||
Other |
(1,538 |
) |
(4,305 |
) |
|||
Deferred income tax liabilities |
(405,198 |
) |
(181,379 |
) |
|||
Net deferred income tax liabilities |
(183,889 |
) |
(32,253 |
) |
|||
Valuation allowance |
(42,147 |
) |
(131,931 |
) |
|||
Net deferred income tax liabilities |
$ |
(226,036 |
) |
$ |
(164,184 |
) |
|
The changes in deferred income tax assets, liabilities and valuation allowances at December 31, 2015 reflect the acquisition of various legal entities, including the tax attributes. The acquisitions were accounted for under U.S. GAAP as stock acquisitions and business combinations. As of December 31, 2015, we have federal, state and foreign net operating loss carryforwards of approximately $362.4 million, $199.9 million and $126.6 million, respectively, that expire at various dates through 2035. Included in the foreign net operating losses is $112.9 million related to OPKO Biologics. As of December 31, 2015, we have research and development tax credit carryforwards of approximately $7.4 million that expire in varying amounts
105
through 2035. As of each reporting date, management considers new evidence, both positive and negative, that could affect its view of the future realization of deferred tax assets. As a result of the merger with Bio-Reference, OPKO released the full valuation allowance recorded against OPKO’s U.S. deferred tax assets, which resulted in an income tax benefit of $93.4 million.
As a result of certain realization requirements of ASC 718, Compensation - Stock Compensation, the table of deferred tax assets and liabilities shown above does not include certain deferred tax assets as of December 31, 2015 and 2014, that arose directly from (or the use of which was postponed by) tax deductions related to equity compensation that are greater than the compensation recognized for financial reporting. Equity will be increased by $33.9 million if and when such deferred tax assets are ultimately realized. The Company uses ASC 740 ordering when determining when excess tax benefits have been realized.
Under Section 382 of the Internal Revenue Code of 1986, as amended, certain significant changes in ownership may restrict the future utilization of our income tax loss carryforwards and income tax credit carryforwards in the U.S. The annual limitation is equal to the value of our stock immediately before the ownership change, multiplied by the long-term tax-exempt rate (i.e., the highest of the adjusted Federal long-term rates in effect for any month in the three-calendar-month period ending with the calendar month in which the change date occurs). This limitation may be increased under the IRC§ 338 Approach (IRS approved methodology for determining recognized Built-In Gain). As a result, federal net operating losses and tax credits may expire before we are able to fully utilize them.
During 2008, we conducted a study to determine the impact of the various ownership changes that occurred during 2007 and 2008. As a result, we have concluded that the annual utilization of our net operating loss carryforwards (“NOLs”) and tax credits is subject to a limitation pursuant to Internal Revenue Code section 382. Under the tax law, such NOLs and tax credits are subject to expiration from 15 to 20 years after they were generated. As a result of the annual limitation that may be imposed on such tax attributes and the statutory expiration period, some of these tax attributes may expire prior to our being able to use them. There is no current impact on these financial statements as a result of the annual limitation. This study did not conclude as to whether eXegenics’ pre-merger NOLs were limited under Section 382. As such, of the $362.4 million of federal net operating loss carryforwards, at least approximately $50.9 million may not be able to be utilized.
Uncertain Income Tax Positions
We file federal income tax returns in the U.S. and various foreign jurisdictions, as well as with various U.S. states and the Ontario and Quebec provinces in Canada. We are subject to routine tax audits in all jurisdictions for which we file tax returns. Tax audits by their very nature are often complex and can require several years to complete. It is reasonably possible that some audits will close within the next twelve months, which we do not believe would result in a material change to our accrued uncertain tax positions. Additionally, included in income tax expense is an accrual of $2.3 million related to uncertain tax positions involving income recognition from the Pfizer Transaction. We recognize that local tax law is inherently complex and the local taxing authorities may not agree with certain tax positions taken. Consequently, it is reasonably possible that ultimate resolution of these matters in any jurisdiction may be significantly more or less than estimated. We evaluated the estimated tax exposure for a range of current likely outcomes to be from $0 to approximately $50.0 million and recorded our accrual to reflect our best expectation of ultimate resolution.
U.S. Federal: Under the tax statute of limitations applicable to the Internal Revenue Code, we are no longer subject to U.S. federal income tax examinations by the Internal Revenue Service for years before 2012. However, because we are carrying forward income tax attributes, such as net operating losses and tax credits from 2012 and earlier tax years, these attributes can still be audited when utilized on returns filed in the future.
State: Under the statutes of limitation applicable to most state income tax laws, we are no longer subject to state income tax examinations by tax authorities for years before 2012 in states in which we have filed income tax returns. Certain states may take the position that we are subject to income tax in such states even though we have not filed income tax returns in such states and, depending on the varying state income tax statutes and administrative practices, the statute of limitations in such states may extend to years before 2012.
Foreign: Under the statutes of limitations applicable to our foreign operations, we are generally no longer subject to tax examination for years before 2010 in jurisdictions where we have filed income tax returns.
106
Unrecognized Tax Benefits
As of December 31, 2015, 2014, and 2013, the total amount of gross unrecognized tax benefits was approximately $8.6 million, $5.9 million, and $9.2 million, respectively. As of December 31, 2015, the total gross unrecognized tax benefit of $8.6 million consisted of increases of $3.5 million as a result of current year activity, and decreases of $0.8 million as a result of the lapse of statutes of limitations. As of December 31, 2015, the total amount of unrecognized tax benefits that, if recognized, would affect our effective income tax rate was $0.7 million. We account for any applicable interest and penalties on uncertain tax positions as a component of income tax expense. As of December 31, 2014 and 2013, $0.9 million and $0.2 million of the unrecognized tax benefits, if recognized, would have affected our effective income tax rate. We believe it is reasonably possible that approximately $0.1 million of unrecognized tax benefits may be recognized within the next twelve months.
The following summarizes the changes in our gross unrecognized income tax benefits.
For the years ended December 31, |
|||||||||||
(In thousands) |
2015 |
2014 |
2013 |
||||||||
Unrecognized tax benefits at beginning of period |
$ |
5,890 |
$ |
9,231 |
$ |
9,245 |
|||||
Gross increases – tax positions in prior period |
955 |
524 |
58 |
||||||||
Gross increases – tax positions in current period |
2,543 |
193 |
517 |
||||||||
Gross decreases – tax positions in prior period |
(176 |
) |
(396 |
) |
(589 |
) |
|||||
Lapse of Statute of Limitations |
(617 |
) |
(472 |
) |
— |
||||||
Settlements |
— |
(3,190 |
) |
— |
|||||||
Unrecognized tax benefits at end of period |
$ |
8,595 |
$ |
5,890 |
$ |
9,231 |
|||||
Other Income Tax Disclosures
The significant elements contributing to the difference between the federal statutory tax rate and the effective tax rate are as follows:
For the years ended December 31, |
||||||||
2015 |
2014 |
2013 |
||||||
Federal statutory rate |
35.0 |
% |
35.0 |
% |
35.0 |
% |
||
State income taxes, net of federal benefit |
2.8 |
% |
2.5 |
% |
2.4 |
% |
||
Foreign income tax |
(7.8 |
)% |
(10.3 |
)% |
(7.9 |
)% |
||
Research and development tax credits |
— |
% |
1.1 |
% |
1.0 |
% |
||
Non-Deductible components of Convertible Debt |
(9.4 |
)% |
(3.8 |
)% |
(16.7 |
)% |
||
Valuation allowance |
61.1 |
% |
(25.3 |
)% |
(11.4 |
)% |
||
Other |
(1.7 |
)% |
0.8 |
% |
(3.9 |
)% |
||
Total |
80.0 |
% |
— |
% |
(1.5 |
)% |
||
The following table reconciles our losses before income taxes between U.S. and foreign jurisdictions:
For the years ended December 31, |
|||||||||||
(In thousands) |
2015 |
2014 |
2013 |
||||||||
Pre-tax loss: |
|||||||||||
U.S. |
$ |
(113,612 |
) |
$ |
(84,075 |
) |
$ |
(74,861 |
) |
||
Foreign |
(30,091 |
) |
(87,567 |
) |
(37,874 |
) |
|||||
Total |
$ |
(143,703 |
) |
$ |
(171,642 |
) |
$ |
(112,735 |
) |
||
No additional provision has been made for U.S. or foreign income taxes on the undistributed earnings of subsidiaries or for unrecognized deferred tax liabilities for temporary differences related to investments in subsidiaries, as such earnings are expected to be permanently reinvested.
Note 11 Related Party Transactions
107
In February 2014, Dr. Frost, our Chairman and Chief Executive Officer, paid a filing fee of $280,000 to the Federal Trade Commission (the “FTC”) under the Hart-Scott-Rodino Antitrust Improvements Act of 1976 (“HSR Act”) in connection with filings made by us and Dr. Frost. We reimbursed Dr. Frost for the HSR filing fee.
In October, 2013, we paid the $170,000 filing fee to the FTC in connection with filings made by us and Dr. Hsiao, our Vice Chairman of the Board and Chief Technical Officer, under the HSR Act.
We hold investments in Zebra (ownership 29%), Sevion (3%), Neovasc (4%), ChromaDex Corporation (2%), MabVax (1%), and ARNO (4%). These investments were considered related party transactions as a result of our executive management’s ownership interests and/or board representation in these entities. See further discussion of our investments in Note 4. In July 2015, we made an additional $500 thousand investment in a private placement transaction with Sevion pursuant to which we acquired 66,667 shares of Series C Convertible Preferred Stock convertible into 666,667 shares of common stock and warrants to purchase 333,333 shares of common stock. In October 2015, we made an additional $375 thousand investment in MabVax pursuant to which we acquired 340,909 shares of common stock at $1.10 and 170,454 warrants to purchase shares of common stock. In November 2015, we made an additional $1.0 million investment in Zebra pursuant to which we acquired 420,000 shares of Series A-2 Preferred Stock.
In August 2013, we acquired OPKO Biologics (formerly PROLOR) pursuant to an Agreement and Plan of Merger dated as of April 23, 2013 in an all-stock transaction. Until completion of the acquisition, Dr. Frost was PROLOR’s Chairman of the Board and a greater than 5% stockholder of PROLOR. Dr. Hsiao and Mr. Rubin were also directors and less than 5% stockholders of PROLOR.
In January 2013, we sold $175.0 million aggregate principal amount of 2033 Senior Notes in a private placement in reliance on exemptions from registration under the Securities Act. The Purchasers of the 2033 Senior Notes include the Gamma Trust and Hsu Gamma. The 2033 Senior Notes were issued on January 30, 2013.
During the years ended December 31, 2014, and 2013, FineTech recorded revenue of $0.3 million and $0.3 million, respectively, for the sale of APIs to Teva Pharmaceutical Industries, Limited (“Teva”). Dr. Frost previously served as the Chairman of the Board of Directors of Teva until 2015. No revenue was recorded for the year ended December 31, 2015.
In 2012, we made a $1.7 million investment in Biozone. Effective January 2, 2014, Biozone completed a merger with Cocrystal Discovery, Inc. (“Cocrystal”), another entity in which we had an equity investment. The name of the issuer was changed to Cocrystal Pharma, Inc. (“COCP”). Dr. Frost previously invested in both Biozone and Cocrystal. Effective January 16, 2014, we invested an additional $0.5 million in the company as part of a $2.75 million private placement and received 1.0 million shares of common stock and 1.0 million 10-year warrants exercisable at $0.50 per share. At December 31, 2015, we hold an 8% ownership interest in COCP.
We lease office space from Frost Real Estate Holdings, LLC (“Frost Holdings”) in Miami, Florida, where our principal executive offices are located. Effective May 28, 2015, we entered into an amendment to our lease agreement with Frost Holdings. The lease, as amended, is for approximately 25,000 square feet of space. The lease provides for payments of approximately $66 thousand per month in the first year increasing annually to $75 thousand per month in the fifth year, plus applicable sales taxes. The rent is inclusive of operating expenses, property taxes and parking. The rent was reduced by $216 thousand for the cost of tenant improvements.
Our wholly-owned subsidiary, Bio-Reference purchases and uses certain products acquired from InCellDx, Inc., a company in which we hold a 27% minority interest in.
We reimburse Dr. Frost for Company-related use by Dr. Frost and our other executives of an airplane owned by a company that is beneficially owned by Dr. Frost. Prior to 2015, we reimbursed Dr. Frost in an amount equal to the cost of a first class airline ticket between the travel cities for each executive, including Dr. Frost, traveling on the airplane for Company-related business. Beginning in the first quarter of 2015, we reimburse Dr. Frost for out-of-pocket operating costs for the use of the airplane by Dr. Frost or Company executives for Company-related business. We do not reimburse Dr. Frost for personal use of the airplane by Dr. Frost or any other executive. For the years ended December 31, 2015, 2014, and 2013, we recognized approximately $595 thousand, $175 thousand, and $93 thousand, respectively, for Company-related travel by Dr. Frost and other OPKO executives.
108
Note 12 Employee Benefit Plans
Effective January 1, 2007, the OPKO Health Savings and Retirement Plan (the “Plan”) permits employees to contribute up to 100% of qualified pre-tax annual compensation up to annual statutory limitations. The discretionary company match for employee contributions to the Plan is 100% up to the first 4% of the participant’s earnings contributed to the Plan. Our matching contributions to the Plan were approximately $0.8 million, $0.6 million and $0.5 million for the years ended December 31, 2015, 2014, and 2013 respectively.
Bio-Reference Laboratories, Inc. sponsors a 401(k) Profit-Sharing Plan (the “Plan”). Employees become eligible for participation after attaining the age of eighteen and completing one year of service. Participants may elect to contribute up to 60% of their compensation, as defined in the Plan, to a maximum allowed by the Internal Revenue Service. Bio-Reference makes a matching contribution to the plan for each participant who has elected to make tax-deferred contributions. The discretionary company match for employee contributions to the Plan is 100% up to the first 3% of the participant’s earnings contributed to the Plan, with an annual maximum match of $1 thousand. Bio-Reference Laboratories, Inc. elected to make a matching contribution which amounted to $1.5 million for the year ended December 31, 2015.
GeneDx, Inc. sponsors a 401(k) Profit-Sharing Plan (the “Plan”). Employees become eligible for participation after attaining the age of eighteen and completing one month of service. Participants may elect to contribute up to 100% of their compensation, as defined in the Plan, to a maximum allowed by the Internal Revenue Service. GeneDx, Inc. makes a matching contribution to the plan for each participant who has elected to make tax-deferred contributions. The discretionary company match for employee contributions to the Plan is 100% up to the first 3%, plus 50% of the next 2% of the participant’s earnings contributed to the Plan. GeneDx, Inc. elected to make a matching contribution which amounted to $0.8 million for the year ended December 31, 2015.
Note 13 Commitments and Contingencies
In connection with our acquisitions of CURNA, OPKO Diagnostics, OPKO Health Europe and OPKO Renal, we agreed to pay future consideration to the sellers upon the achievement of certain events. As a result, as of December 31, 2015, we recorded $54.4 million as contingent consideration, with $22.2 million recorded within Accrued expenses and $32.3 million recorded within Other long-term liabilities in the accompanying Consolidated Balance Sheets. Refer to Note 5. During the year ended December 31, 2015, we satisfied a $20.0 million contingent payment to the former owners of OPKO Renal through the issuance of 1,194,337 shares of our common stock in the third quarter of 2015.
In July 2012, OPKO Lab received a letter from AdvanceMed Corporation (“AdvanceMed”) regarding a post-payment review conducted by AdvanceMed (the “Post-Payment Review Letter”). The Post-Payment Review Letter originated with a post payment review audit by AdvanceMed of 183 claims submitted by OPKO Lab to the Medicare program. OPKO Lab believes that its billing practices were appropriate and it is following the appeal process set forth by Medicare. OPKO Lab received a partially favorable determination, which reduced the amount of the alleged overpayment, and it continues to appeal the remaining alleged overpayments. No assurances can be given about the outcome of the appeal.
On or around October 21, 2014, we received a Civil Investigative Demand (“Demand”) from the U.S. Attorney’s Office for the Middle District of Tennessee (“Attorney’s Office”). The Demand concerns an investigation of allegations that the Company or one of its affiliated entities or other parties submitted false claims for payment related to services provided to government healthcare program beneficiaries in violation of the False Claims Act, 31 U.S.C. Section 3729. We are fully cooperating with the investigation and are producing documents responsive to the Demand. It is too early to assess the range of loss, if any.
Following the announcement of entry into an agreement and plan of merger with Bio-Reference, four putative class action complaints challenging the merger were filed in the Superior Court of New Jersey in Bergen County (the “Court”). The parties executed a stipulated consent order that the actions would be consolidated for all purposes, including trial, in the Chancery Division under Docket No. C-207-15, bearing the caption In re Bio-Reference Laboratories, Inc. Shareholder Litigation (the “Consolidated Action”). The complaints name Bio-Reference, OPKO, a wholly-owned merger subsidiary of OPKO (“Merger Sub”) and members of the Bio-Reference board as defendants. The complaints generally allege, among other things, that members of the Bio-Reference board breached their fiduciary duties to Bio-Reference’s shareholders by agreeing to sell Bio-Reference for an inadequate price and agreeing to inappropriate deal protection provisions in the merger agreement that may preclude Bio-Reference from soliciting any potential acquirers and limit the ability of the Bio-Reference board to act with respect to investigating and pursuing superior proposals and alternatives. In August, the parties executed a memorandum of understanding reflecting terms of a settlement, which was replaced in September 2015 by a stipulation and agreement of compromise, settlement and release resolving all matters between them. In January 2016, the Court entered an order finally
109
approving the settlement. The settlement did not have a material impact on our business, financial condition, results of operations or cash flows.
Under a license agreement one of our subsidiaries has with Washington University in St. Louis, we are obligated to pay Washington University a single digit percentage of any sublicensing payment we receive in connection with a sublicense of our rights to Washington University patents subject to certain exceptions. In connection with the Pfizer Transaction, we sublicensed to Pfizer the sole remaining patent licensed to us by Washington University and paid to Washington University the sublicensing payment we believe is due under the license agreement. Washington University has questioned the computation of the sublicense payment and has notified us that it would like to review additional information relating to the sublicense and the Pfizer Transaction to determine whether additional amounts are owed to it.
We accrue a liability for legal contingencies when we believe that it is both probable that a liability has been incurred and that we can reasonably estimate the amount of the loss. We review these accruals and adjust them to reflect ongoing negotiations, settlements, rulings, advice of legal counsel and other relevant information. To the extent new information is obtained and our views on the probable outcomes of claims, suits, assessments, investigations or legal proceedings change, changes in our accrued liabilities would be recorded in the period in which such determination is made. For the matters referenced in the paragraph below, the amount of liability is not probable or the amount cannot be reasonably estimated; and, therefore, accruals have not been made. In addition, in accordance with the relevant authoritative guidance, for matters which the likelihood of material loss is at least reasonably possible, we provide disclosure of the possible loss or range of loss; however, if a reasonable estimate cannot be made, we will provide disclosure to that effect.
We are a party to other litigation in the ordinary course of business. We do not believe that any such litigation will have a material adverse effect on our business, financial condition, results of operations or cash flows.
We expect to incur substantial losses as we continue the development of our product candidates, continue our other research and development activities, and establish a pharmaceutical sales and marketing infrastructure in anticipation of the commercialization of our pharmaceutical product candidates. We currently have limited pharmaceutical commercialization capabilities, and it is possible that we may never successfully commercialize any of our diagnostic and pharmaceutical product candidates. We do not currently generate significant revenue from any of our diagnostic and pharmaceutical product candidates. Our research and development activities are budgeted to expand over a period of time and will require further resources if we are to be successful. As a result, we believe that our operating losses are likely to be substantial over the next several years. We may need to obtain additional funds to further develop our research and development programs, and there can be no assurance that additional capital will be available to us on acceptable terms, or at all.
We have employment agreements with certain executives which provide for compensation and certain other benefits and for severance payments under certain circumstances.
At December 31, 2015, we were committed to make future purchases for inventory and other items in 2016 that occur in the ordinary course of business under various purchase arrangements with fixed purchase provisions aggregating $48.3 million.
Note 14 Strategic Alliances
Pfizer Inc.
We plan to develop a portfolio of product candidates through a combination of internal development and external partnerships. In December 2014, we entered into an exclusive worldwide agreement with Pfizer Inc. (“Pfizer”) for the development and commercialization of our long-acting hGH-CTP for the treatment of growth hormone deficiency (“GHD”) in adults and children, as well as for the treatment of growth failure in children born small for gestational age (“SGA”) (the “Pfizer Transaction”).
The Pfizer Transaction closed in January 2015 following the termination of the waiting period under the Hart-Scott-Rodino Act. Under the terms of the Pfizer Transaction, we received non-refundable and non-creditable upfront payments of $295.0 million and are eligible to receive up to an additional $275.0 million upon the achievement of certain regulatory milestones. Pfizer received the exclusive license to commercialize hGH-CTP worldwide. In addition, we are eligible to receive initial tiered royalty payments associated with the commercialization of hGH-CTP for Adult GHD with percentage rates ranging from the high teens to mid-twenties. Upon the launch of hGH-CTP for Pediatric GHD in certain major markets, the royalties will transition to regional, tiered gross profit sharing for both hGH-CTP and Pfizer’s Genotropin®.
110
The agreement with Pfizer will remain in effect until the last sale of the licensed product, unless earlier terminated as permitted under the agreement. In addition to termination rights for material breach and bankruptcy, Pfizer is permitted to terminate the Agreement in its entirety, or with respect to one or more world regions, without cause after a specified notice period. If the Agreement is terminated by us for Pfizer’s uncured material breach, or by Pfizer without cause, provision has been made for transition of product and product responsibilities to us for the terminated regions, as well as continued supply of product by Pfizer or transfer of supply to us in order to support the terminated regions.
We will lead the clinical activities and will be responsible for funding the development programs for the key indications, which includes Adult and Pediatric GHD and Pediatric SGA. Pfizer will be responsible for all development costs for additional indications as well as all post-marketing studies. In addition, Pfizer will fund the commercialization activities for all indications and lead the manufacturing activities covered by the global development plan.
For revenue recognition purposes, we viewed the Pfizer Transaction as a multiple-element arrangement. Multiple-element arrangements are analyzed to determine whether the various performance obligations, or elements, can be separated or whether they must be accounted for as a single unit of accounting. We evaluated whether a delivered element under an arrangement has standalone value and qualifies for treatment as a separate unit of accounting. Deliverables that do not meet these criteria are not evaluated separately for the purpose of revenue recognition. For a single unit of accounting, payments received are recognized in a manner consistent with the final deliverable. We determined that the deliverables under the Pfizer Transaction, including the licenses granted to Pfizer, as well as our obligations to provide various research and development services, will be accounted for as a single unit of account. This determination was made because the ongoing research and development services to be provided by us are essential to the overall arrangement as we have significant knowledge and technical know-how that is important to realizing the value of the licenses granted. The performance period over which the revenue will be recognized is expected to continue from the first quarter of 2015 through 2019, when we anticipate completing the various research and development services that are specified in the Pfizer Transaction and our performance obligations are completed. We will continue to review the timing of when our research and development services will be completed in order to assess that the estimated performance period over which the revenue is to be recognized is appropriate. Any significant changes in the timing of the performance period will result in a change in the revenue recognition period.
We are recognizing the non-refundable $295.0 million upfront payments on a straight-line basis over the performance period. We recognized $65.5 million of revenue related to the Pfizer Transaction in Revenue from transfer of intellectual property in our Consolidated Statement of Operations during the year ended December 31, 2015, and had deferred revenue related to the Pfizer Transaction of $229.5 million at December 31, 2015. As of December 31, 2015, $70.6 million of deferred revenue related to the Pfizer Transaction was classified in Accrued expenses and $158.9 million was classified in Other long-term liabilities in our Consolidated Balance Sheet. During the year ended December 31, 2015, we incurred $55.3 million in research and development expenses related to hGH-CTP.
The Pfizer Transaction includes milestone payments of $275.0 million upon the achievement of certain milestones. The milestones range from $20.0 million to $90.0 million each and are based on achievement of regulatory approval in the U.S. and regulatory approval and price approval in other major markets. We evaluated each of these milestone payments and believe that all of the milestones are substantive as (i) there is substantive uncertainty at the close of the Pfizer Transaction that the milestones would be achieved as approval from a regulatory authority must be received to achieve the milestones which would be commensurate with the enhancement of value of the underlying intellectual property, (ii) the milestones relate solely to past performance and (iii) the amount of the milestone is reasonable in relation to the effort expended and the risk associated with the achievement of the milestone. The milestone payments will be recognized as revenue in full in the period in which the associated milestone is achieved, assuming all other revenue recognition criteria are met. To date, no revenue has been recognized related to the achievement of the milestones.
In the first quarter of 2015, we made a payment of $25.9 million to the Office of the Chief Scientist of the Israeli Ministry of Economy (“OCS”) in connection with repayment obligations resulting from grants previously made by the OCS to OPKO Biologics to support development of hGH-CTP and the outlicense of the technology outside of Israel. We recognized the $25.9 million payment in Grant repayment expense in our Consolidated Statement of Operations during the year ended December 31, 2015.
TESARO
In November 2009, we entered into an asset purchase agreement (the “NK-1 Agreement”) under which we acquired VARUBI™ (rolapitant) and other neurokinin-1 (“NK-1”) assets from Merck. In December 2010, we entered into an exclusive license agreement with TESARO, in which we out-licensed the development, manufacture, commercialization and distribution of our lead NK-1 candidate, VARUBI™ (the “TESARO License”). Under the terms of the license, we received a $6.0 million upfront payment from TESARO and are eligible to receive milestone payments of up to $30.0 million upon achievement of
111
certain regulatory and commercial sale milestones (of which $20.0 million has been received to date) and additional commercial milestone payments of up to $85.0 million if specified levels of annual net sales are achieved. During the years ended December 31, 2015 and 2014, $15.0 million and $5.0 million of revenue, respectively, has been recognized related to the achievement of the milestones under the TESARO License. TESARO is also obligated to pay us tiered royalties on annual net sales achieved in the United States and Europe at percentage rates that range from the low double digits to the low twenties, and outside of the United States and Europe at low double-digit percentage rates. TESARO assumed responsibility for clinical development and commercialization of licensed products at its expense. Under the Agreement, we will continue to receive royalties on a country-by-country and product-by-product basis until the later of the date that all of the patent rights licensed from us and covering VARUBI™ expire, are invalidated or are not enforceable and 12 years from the first commercial sale of the product.
If TESARO elects to develop and commercialize VARUBI™ in Japan through a third-party licensee, TESARO will share equally with us all amounts it receives in connection with such activities, subject to certain exceptions and deductions. In addition, we will have an option to market the products in Latin America.
The term of the license will remain in force until the expiration of the royalty term in each country, unless we terminate the license earlier for TESARO’s material breach of the license or bankruptcy. TESARO has a right to terminate the license at any time during the term for any reason on three months’ written notice.
TESARO’s New Drug Application (“NDA”) for approval of oral VARUBI™, a neurokinin-1 receptor antagonist in development for the prevention of chemotherapy-induced nausea and vomiting, was approved by the U.S. FDA in September 2015, and in November 2015, TESARO announced the commercial launch of VARUBI™ in the United States. Under the terms of the NK-1 Agreement, upon approval by the FDA of the TESARO’s NDA for oral VARUBI™, we were required to pay Merck a $5.0 million milestone payment. In addition, $5.0 million will be due and payable each year thereafter for the next four (4) years on the anniversary date of the NDA approval. We recognized the present value of the milestone payments on FDA approval of $23.0 million as an intangible asset which will be amortized to expense over the expected useful life of the asset, which is approximately 13 years. The present value of the future payments to Merck of $18.2 million at December 31, 2015 is recorded as a liability in our Consolidated Balance Sheet with $5.0 million in Accrued expenses and $13.2 million in Other long-term liabilities.
Pharmsynthez
In April 2013, we entered into a series of concurrent transactions with Pharmsynthez, a Russian pharmaceutical company traded on the Moscow Stock Exchange pursuant to which we acquired an equity method investment in Pharmsynthez (ownership 17%). We also granted rights to certain technologies in the Russian Federation, Ukraine, Belarus, Azerbaijan and Kazakhstan (the “Territories”) to Pharmsynthez and agreed to perform certain development activities. We will receive from Pharmsynthez royalties on net sales of products incorporating the technologies in the Territories, as well as a percentage of any sublicense income from third parties for the technologies in the Territories.
In July 2015, we entered into a Note Purchase Agreement with Pharmsynthez pursuant to which we delivered $3.0 million to Pharmsynthez in exchange for a $3.0 million note (the “Pharmsynthez Note Receivable”). The Pharmsynthez Note Receivable is due on or before July 1, 2016, and Pharmsynthez may satisfy the note either in cash or shares of its capital stock. We recorded the Pharmsynthez Note Receivable within Prepaid expenses and other current assets in our Consolidated Balance Sheet.
RXi Pharmaceuticals Corporation
In March 2013, we completed the sale to RXi of substantially all of our assets in the field of RNA interference (the “RNAi Assets”) (collectively, the “Asset Purchase Agreement”). In accounting for the sale of the RNAi Assets, we determined that we did not have any continuing involvement in the development of the RNAi Assets or any other future performance obligations and, as a result, during the year ended December 31, 2013, we recognized $12.5 million of Revenue from transfer of intellectual property in our Consolidated Statement of Operations.
Pursuant to the Asset Purchase Agreement, RXi will be required to pay us up to $50.0 million in milestone payments upon the successful development and commercialization of each drug developed by RXi, certain of its affiliates or any of its or their licensees or sublicensees utilizing patents included within the RNAi Assets (each, a “Qualified Drug”). In addition, RXi will also be required to pay us royalties equal to: (a) a mid single-digit percentage of “Net Sales” (as defined in the Asset Purchase Agreement) with respect to each Qualified Drug sold for an ophthalmologic use during the applicable “Royalty Period” (as defined in the Asset Purchase Agreement); and (b) a low single-digit percentage of net sales with respect to each Qualified Drug sold for a non-ophthalmologic use during the applicable royalty period.
112
Other
We have completed strategic deals with UT Southwestern, Washington University, INEOS Healthcare, TSRI, the President and Fellows of Harvard College, and Academia Sinica, among others. In connection with these agreements, upon the achievement of certain milestones we are obligated to make certain payments and have royalty obligations upon sales of products developed under the license agreements. At this time, we are unable to estimate the timing and amounts of payments as the obligations are based on future development of the licensed products.
113
Note 15 Leases
Operating Leases
We conduct certain of our operations under operating lease agreements. Rent expense under operating leases was approximately $7.8 million, $2.6 million, and $1.9 million for the years ended December 31, 2015, 2014, and 2013, respectively.
As of December 31, 2015, the aggregate future minimum lease payments under all non-cancelable operating leases with initial or remaining lease terms in excess of one year are as follows:
Year Ending |
(In thousands) |
||
2016 |
$ |
15,830 |
|
2017 |
10,749 |
||
2018 |
7,862 |
||
2019 |
6,558 |
||
2020 |
3,208 |
||
Thereafter |
7,525 |
||
Total minimum operating lease commitments |
$ |
51,732 |
|
Capital Leases
We acquired various assets under capital leases in connection with our acquisition of Bio-Reference in August 2015. Capital leases are included within Property, plant and equipment, net in our Consolidated Balance Sheet with interest rates ranging from 2% to 7% as follows:
Capital leases |
Year ended December 31, 2015 |
||
Medical Equipment |
$ |
50,139 |
|
Automobiles |
6,748 |
||
Total |
56,887 |
||
Less: Accumulated Depreciation |
(6,798 |
) |
|
Net capital leases in Property, plant and equipment |
$ |
50,089 |
|
As of December 31, 2015, the aggregate future minimum lease payments under all non-cancelable capital leases with initial or remaining lease terms in excess of one year are as follows:
Year Ending |
(In thousands) |
||
2016 |
$ |
5,762 |
|
2017 |
3,951 |
||
2018 |
2,607 |
||
2019 |
1,386 |
||
2020 |
603 |
||
Thereafter |
794 |
||
Total minimum capital lease commitments |
$ |
15,103 |
|
Less interest: |
$ |
445 |
|
Present value of minimum lease payments |
$ |
14,658 |
|
114
Note 16 Segments
We currently manage our operations in two reportable segments, pharmaceutical and diagnostics. The pharmaceutical segment consists of our pharmaceutical operations we acquired in Chile, Mexico, Ireland, Israel and Spain and our pharmaceutical research and development. The diagnostics segment primarily consists of our clinical laboratory operations we acquired through the acquisitions of Bio-Reference and OPKO Lab and our point-of-care operations. There are no significant inter-segment sales. We evaluate the performance of each segment based on operating profit or loss. There is no inter-segment allocation of interest expense and income taxes.
Information regarding our operations and assets for our operating segments and the unallocated corporate operations as well as geographic information are as follows:
115
For the years ended December 31, |
|||||||||||
(In thousands) |
2015 |
2014 |
2013 |
||||||||
Revenue from services: |
|||||||||||
Pharmaceutical |
$ |
— |
$ |
— |
$ |
— |
|||||
Diagnostics |
329,599 |
8,426 |
10,833 |
||||||||
Corporate |
140 |
240 |
825 |
||||||||
$ |
329,739 |
$ |
8,666 |
$ |
11,658 |
||||||
Product revenues: |
|||||||||||
Pharmaceutical |
$ |
80,146 |
$ |
76,983 |
$ |
68,161 |
|||||
Diagnostics |
— |
— |
— |
||||||||
Corporate |
— |
— |
— |
||||||||
$ |
80,146 |
$ |
76,983 |
$ |
68,161 |
||||||
Revenue from transfer of intellectual property: |
|||||||||||
Pharmaceutical |
$ |
81,853 |
$ |
5,285 |
$ |
15,160 |
|||||
Diagnostics |
— |
191 |
1,551 |
||||||||
Corporate |
— |
— |
— |
||||||||
$ |
81,853 |
$ |
5,476 |
$ |
16,711 |
||||||
Operating (loss) income: |
|||||||||||
Pharmaceutical |
$ |
(40,395 |
) |
$ |
(94,401 |
) |
$ |
(29,809 |
) |
||
Diagnostics |
(10,294 |
) |
(21,647 |
) |
(22,199 |
) |
|||||
Corporate |
(46,512 |
) |
(27,725 |
) |
(24,473 |
) |
|||||
Less: Operating loss attributable to noncontrolling interests |
(1,280 |
) |
(2,042 |
) |
(3,151 |
) |
|||||
$ |
(98,481 |
) |
$ |
(145,815 |
) |
$ |
(79,632 |
) |
|||
Depreciation and amortization: |
|||||||||||
Pharmaceutical |
$ |
10,245 |
$ |
7,936 |
$ |
8,234 |
|||||
Diagnostics |
31,918 |
6,894 |
6,833 |
||||||||
Corporate |
85 |
97 |
149 |
||||||||
$ |
42,248 |
$ |
14,927 |
$ |
15,216 |
||||||
Net loss from investment in investees: |
|||||||||||
Pharmaceutical |
$ |
(7,105 |
) |
$ |
(3,587 |
) |
$ |
(11,456 |
) |
||
Diagnostics |
— |
— |
— |
||||||||
Corporate |
— |
— |
— |
||||||||
$ |
(7,105 |
) |
$ |
(3,587 |
) |
$ |
(11,456 |
) |
|||
Revenues: |
|||||||||||
United States |
$ |
344,464 |
$ |
14,142 |
$ |
28,369 |
|||||
Ireland |
78,989 |
— |
— |
||||||||
Chile |
29,885 |
29,154 |
31,650 |
||||||||
Spain |
16,622 |
21,323 |
18,800 |
||||||||
Israel |
18,107 |
20,638 |
13,252 |
||||||||
Mexico |
3,671 |
5,807 |
4,459 |
||||||||
Other |
— |
61 |
— |
||||||||
$ |
491,738 |
$ |
91,125 |
$ |
96,530 |
||||||
116
(In thousands) |
December 31, 2015 |
December 31, 2014 |
|||||
Assets: |
|||||||
Pharmaceutical |
$ |
1,258,011 |
$ |
1,064,498 |
|||
Diagnostics |
1,479,841 |
108,072 |
|||||
Corporate |
61,762 |
95,094 |
|||||
$ |
2,799,614 |
$ |
1,267,664 |
||||
Goodwill: |
|||||||
Pharmaceutical |
$ |
251,225 |
$ |
173,327 |
|||
Diagnostics |
492,123 |
50,965 |
|||||
Corporate |
— |
— |
|||||
$ |
743,348 |
$ |
224,292 |
||||
During the year ended December 31, 2015, revenue recognized under the Pfizer Transaction represented 13% of our total revenue. During the year ended December 31, 2014, one customer of our pharmaceutical segment represented 13% of our total revenue. During the year ended December 31, 2013, no customer represented more than 10% of our total revenue. As of December 31, 2015, one customer represented more than 10% of our accounts receivable balance. As of December 31, 2014 and 2013, no customer represented more than 10% of our accounts receivable balance.
The following table reconciles our Property, plant and equipment, net between U.S. and foreign jurisdictions:
(In thousands) |
December 31, 2015 |
December 31, 2014 |
|||||
PP&E: |
|||||||
U.S. |
$ |
113,307 |
$ |
4,286 |
|||
Foreign |
18,491 |
12,125 |
|||||
Total |
$ |
131,798 |
$ |
16,411 |
|||
Note 17 Fair Value Measurements
We record fair values at an exit price, representing the amount that would be received to sell an asset or paid to transfer a liability in an orderly transaction between market participants. As such, fair value is a market-based measurement that should be determined based on assumptions that market participants would use in pricing an asset or liability. We utilize a three-tier fair value hierarchy, which prioritizes the inputs used in measuring fair value. These tiers include: Level 1, defined as observable inputs such as quoted prices in active markets; Level 2, defined as inputs other than quoted prices in active markets that are either directly or indirectly observable; and Level 3, defined as unobservable inputs in which little or no market data exists, therefore requiring an entity to develop its own assumptions.
A summary of our investments classified as available for sale and carried at fair value, is as follows:
As of December 31, 2015 |
|||||||||||||||
(In thousands) |
Amortized
Cost
|
Gross
unrealized
gains in
Accumulated
OCI
|
Gross
unrealized
losses in
Accumulated
OCI
|
Fair
value
|
|||||||||||
Common stock investments, available for sale |
$ |
2,978 |
$ |
904 |
$ |
(267 |
) |
$ |
3,615 |
||||||
Total assets |
$ |
2,978 |
$ |
904 |
$ |
(267 |
) |
$ |
3,615 |
||||||
117
As of December 31, 2014 |
|||||||||||||||
(In thousands) |
Amortized
Cost
|
Gross
unrealized
gains in
Accumulated
OCI
|
Gross
unrealized
losses in
Accumulated
OCI
|
Fair
value
|
|||||||||||
Common stock investments, available for sale |
$ |
10,038 |
$ |
293 |
$ |
(4,573 |
) |
$ |
5,758 |
||||||
Total assets |
$ |
10,038 |
$ |
293 |
$ |
(4,573 |
) |
$ |
5,758 |
||||||
Any future fluctuation in fair value related to our available for sale investments that is judged to be temporary, and any recoveries of previous write-downs, will be recorded in Accumulated other comprehensive income or loss. If we determine that any future valuation adjustment was other-than-temporary, we will record a loss during the period such determination is made. Any future changes in the fair value of option and warrant instruments will be recorded in Fair value changes of derivative instruments, net in our Consolidated Statements of Operations.
As of December 31, 2015, we have money market funds that qualify as cash equivalents, forward foreign currency exchange contracts for inventory purchases (Refer to Note 18) and contingent consideration related to the acquisitions of CURNA, OPKO Diagnostics, OPKO Health Europe, and OPKO Renal that are required to be measured at fair value on a recurring basis. In addition, in connection with our investment and our consulting agreement with Neovasc, we record the related Neovasc options at fair value as well as the warrants from COCP, ARNO, Sevion and MabVax.
Our financial assets and liabilities measured at fair value on a recurring basis are as follows:
Fair value measurements as of December 31, 2015 |
|||||||||||||||
(In thousands) |
Quoted
prices in
active
markets for
identical
assets
(Level 1)
|
Significant
other
observable
inputs
(Level 2)
|
Significant
unobservable
inputs
(Level 3)
|
Total |
|||||||||||
Assets: |
|||||||||||||||
Money market funds |
$ |
84,421 |
$ |
— |
$ |
— |
$ |
84,421 |
|||||||
Common stock investments, available for sale |
3,615 |
— |
— |
3,615 |
|||||||||||
Common stock options/warrants |
— |
5,338 |
— |
5,338 |
|||||||||||
Forward contracts |
— |
9 |
— |
9 |
|||||||||||
Total assets |
$ |
88,036 |
$ |
5,347 |
$ |
— |
$ |
93,383 |
|||||||
Liabilities: |
|||||||||||||||
Embedded conversion option |
$ |
— |
$ |
— |
$ |
23,737 |
$ |
23,737 |
|||||||
Contingent consideration: |
|||||||||||||||
CURNA |
— |
— |
411 |
411 |
|||||||||||
OPKO Diagnostics |
— |
— |
12,141 |
12,141 |
|||||||||||
OPKO Renal |
— |
— |
41,400 |
41,400 |
|||||||||||
OPKO Health Europe |
— |
— |
470 |
470 |
|||||||||||
Total liabilities |
$ |
— |
$ |
— |
$ |
78,159 |
$ |
78,159 |
|||||||
118
Fair value measurements as of December 31, 2014 |
|||||||||||||||
(In thousands) |
Quoted
prices in
active
markets for
identical
assets
(Level 1)
|
Significant
other
observable
inputs
(Level 2)
|
Significant
unobservable
inputs
(Level 3)
|
Total |
|||||||||||
Assets: |
|||||||||||||||
Money market funds |
$ |
71,286 |
$ |
— |
$ |
— |
$ |
71,286 |
|||||||
Common stock investments, available for sale |
5,758 |
— |
— |
5,758 |
|||||||||||
Common stock options/warrants |
— |
6,314 |
— |
6,314 |
|||||||||||
Forward contracts |
— |
36 |
— |
36 |
|||||||||||
Total assets |
$ |
77,044 |
$ |
6,350 |
$ |
— |
$ |
83,394 |
|||||||
Liabilities: |
|||||||||||||||
Embedded conversion option |
$ |
— |
$ |
— |
$ |
65,947 |
$ |
65,947 |
|||||||
Contingent consideration: |
|||||||||||||||
CURNA |
— |
— |
440 |
440 |
|||||||||||
OPKO Diagnostics |
— |
— |
13,578 |
13,578 |
|||||||||||
OPKO Renal |
— |
— |
55,780 |
55,780 |
|||||||||||
OPKO Health Europe |
— |
— |
1,769 |
1,769 |
|||||||||||
Total liabilities |
$ |
— |
$ |
— |
$ |
137,514 |
$ |
137,514 |
|||||||
The carrying amount and estimated fair value of our 2033 Senior Notes without the embedded conversion option, as well as the applicable fair value hierarchy tiers, are contained in the table below. The fair value of the 2033 Senior Notes is determined using a binomial lattice approach in order to estimate the fair value of the embedded derivative in the 2033 Senior Notes. Refer to Note 6.
December 31, 2015 |
|||||||||||||||||||
(In thousands) |
Carrying
Value
|
Total
Fair Value
|
Level 1 |
Level 2 |
Level 3 |
||||||||||||||
2033 Senior Notes |
$ |
25,675 |
$ |
24,647 |
$ |
— |
$ |
— |
$ |
24,647 |
|||||||||
There have been no transfers between Level 1 and Level 2 and no transfers to or from Level 3 of the fair value hierarchy.
December 31, 2014 |
|||||||||||||||||||
(In thousands) |
Carrying
Value
|
Total
Fair Value
|
Level 1 |
Level 2 |
Level 3 |
||||||||||||||
2033 Senior Notes |
$ |
65,507 |
$ |
63,062 |
$ |
— |
$ |
— |
$ |
63,062 |
|||||||||
There have been no transfers between Level 1 and Level 2 and no transfers to or from Level 3 of the fair value hierarchy.
As of December 31, 2015 and 2014, the carrying value of our other assets and liabilities approximates their fair value due to their short-term nature.
The following tables reconcile the beginning and ending balances of our Level 3 assets and liabilities as of December 31, 2015 and 2014:
119
December 31, 2015 |
|||||||
(In thousands) |
Contingent
consideration
|
Embedded
conversion
option
|
|||||
Balance at December 31, 2014 |
$ |
71,567 |
$ |
65,947 |
|||
Total losses (gains) for the period: |
|||||||
Included in results of operations |
5,050 |
36,587 |
|||||
Foreign currency impact |
(269 |
) |
— |
||||
Payments |
(21,926 |
) |
— |
||||
Conversion |
— |
(78,797 |
) |
||||
Balance at December 31, 2015 |
$ |
54,422 |
$ |
23,737 |
|||
December 31, 2014 |
|||||||||||
(In thousands) |
Contingent consideration |
Deferred acquisition payments, net of discount |
Embedded conversion option |
||||||||
Balance at December 31, 2013 |
$ |
71,620 |
$ |
5,465 |
$ |
101,087 |
|||||
Total losses (gains) for the period: |
|||||||||||
Included in results of operations |
24,446 |
(735 |
) |
12,213 |
|||||||
Foreign currency impact |
(130 |
) |
— |
— |
|||||||
Payments |
(24,369 |
) |
(4,730 |
) |
— |
||||||
Conversion |
— |
— |
(47,353 |
) |
|||||||
Balance at December 31, 2014 |
$ |
71,567 |
$ |
— |
$ |
65,947 |
|||||
The estimated fair values of our financial instruments have been determined by using available market information and what we believe to be appropriate valuation methodologies. We use the following methods and assumptions in estimating fair value:
Contingent consideration – We estimate the fair value of the contingent consideration utilizing a discounted cash flow model for the expected payments based on estimated timing and expected revenues. We use several discount rates depending on each type of contingent consideration related to OPKO Diagnostics, CURNA, OPKO Health Europe, OPKO Renal and Merck (VARUBI™) transactions. If estimated future sales were to decrease by 10%, the contingent consideration related to OPKO Renal would decrease by $1.7 million. As of December 31, 2015, of the $54.4 million of contingent consideration, $22.2 million is recorded in Accrued expenses and $32.3 million is recorded in Other long-term liabilities. As of December 31, 2014, of the $71.6 million of contingent consideration, $27.4 million is recorded in Accrued expenses and $44.2 million is recorded in Other long-term liabilities.
Deferred payments – We estimate the fair value of the deferred payments utilizing a discounted cash flow model for the expected payments.
Embedded conversion option – We estimate the fair value of the embedded conversion option related to the 2033 Senior Notes using a binomial lattice model. Refer to Note 6 for detail description of the binomial lattice model and the fair value assumptions used.
Note 18 Derivative Contracts
120
The following table summarizes the fair values and the presentation of our derivative financial instruments in the Consolidated Balance Sheets:
(In thousands) |
Balance Sheet Component |
December 31, 2015 |
December 31, 2014 |
||||||
Derivative financial instruments: |
|||||||||
Common stock options/warrants |
Investments, net |
$ |
5,338 |
$ |
6,314 |
||||
Embedded conversion option |
2033 Senior Notes, net of discount and estimated fair value of embedded derivatives |
$ |
23,737 |
$ |
65,947 |
||||
Forward contracts |
Unrealized gains on forward contracts are recorded in Prepaid expenses and other current assets. Unrealized losses on forward contracts are recorded in Accrued expenses. |
$ |
9 |
$ |
36 |
||||
We enter into foreign currency forward exchange contracts to cover the risk of exposure to exchange rate differences arising from inventory purchases on letters of credit. Under these forward contracts, for any rate above or below the fixed rate, we receive or pay the difference between the spot rate and the fixed rate for the given amount at the settlement date.
To qualify the derivative instrument as a hedge, we are required to meet strict hedge effectiveness and contemporaneous documentation requirements at the initiation of the hedge and assess the hedge effectiveness on an ongoing basis over the life of the hedge. At December 31, 2015 and 2014, our derivative financial instruments do not meet the documentation requirements to be designated as hedges. Accordingly, we recognize the changes in Fair value of derivative instruments, net in our Consolidated Statements of Operations. The following table summarizes the losses and gains recorded for the years ended December 31, 2015 and 2014:
For the years ended December 31, |
|||||||||||
(In thousands) |
2015 |
2014 |
2013 |
||||||||
Derivative gain (loss): |
|||||||||||
Common stock options/warrants |
$ |
(2,854 |
) |
$ |
1,193 |
$ |
6,544 |
||||
2033 Senior Notes |
(36,588 |
) |
(12,213 |
) |
(52,742 |
) |
|||||
Forward contracts |
$ |
359 |
$ |
388 |
$ |
256 |
|||||
Total |
$ |
(39,083 |
) |
$ |
(10,632 |
) |
$ |
(45,942 |
) |
||
Note 19 Selected Quarterly Financial Data (Unaudited)
For the 2015 Quarters Ended |
|||||||||||||||
(In thousands, except per share data) |
March 31 |
June 30 |
September 30 |
December 31 |
|||||||||||
Total revenues |
$ |
30,084 |
$ |
42,429 |
$ |
143,034 |
$ |
276,191 |
|||||||
Total costs and expenses |
86,998 |
67,838 |
151,257 |
284,126 |
|||||||||||
Net income (loss) |
(118,037 |
) |
(43,241 |
) |
128,247 |
1,603 |
|||||||||
Net income (loss) attributable to common shareholders |
(117,112 |
) |
(42,766 |
) |
128,247 |
1,603 |
|||||||||
Earnings (loss) per share, basic |
$ |
(0.26 |
) |
$ |
(0.09 |
) |
$ |
0.26 |
$ |
— |
|||||
Earnings (loss) per share, diluted |
$ |
(0.26 |
) |
$ |
(0.09 |
) |
$ |
0.18 |
$ |
— |
|||||
For the 2014 Quarters Ended |
|||||||||||||||
(In thousands, except per share data) |
March 31 |
June 30 |
September 30 |
December 31 |
|||||||||||
Total revenues |
$ |
22,274 |
$ |
23,545 |
$ |
19,773 |
$ |
25,533 |
|||||||
Total costs and expenses |
52,550 |
58,429 |
67,974 |
57,987 |
|||||||||||
Net loss |
(45,088 |
) |
(26,075 |
) |
(50,014 |
) |
(53,461 |
) |
|||||||
Net loss attributable to common shareholders |
(44,548 |
) |
(25,478 |
) |
(48,669 |
) |
(52,971 |
) |
|||||||
Earnings (loss) per share, basic |
$ |
(0.11 |
) |
$ |
(0.06 |
) |
$ |
(0.11 |
) |
$ |
(0.12 |
) |
|||
Earnings (loss) per share, diluted |
$ |
(0.11 |
) |
$ |
(0.08 |
) |
$ |
(0.11 |
) |
$ |
(0.12 |
) |
|||
121
For the third quarter of 2015, we previously reported diluted earnings per share ("EPS") of $0.25. We have corrected the amount to $0.18 to reflect an immaterial adjustment calculation.
Note 20 Subsequent Events
On January 5, 2016, we announced that our 2033 Senior Notes continue to be convertible by holders of such notes. We have elected to satisfy our conversion obligation under the 2033 Senior Notes in shares of our Common Stock. This conversion right has been triggered because the closing price per share of our Common Stock has exceeded $9.19, or 130% of the initial conversion price of $7.07, for at least 20 of 30 consecutive trading days during the period ending on December 31, 2015. The conversion right was previously triggered during the quarters ended March 31, 2015, June 30, 2015 and September 30, 2015. The 2033 Senior Notes will continue to be convertible until March 31, 2016, and may be convertible thereafter, if one or more of the conversion conditions specified in the Indenture, dated as of January 30, 2013, by and between the Company and Wells Fargo Bank N.A., is satisfied during future measurement periods. Pursuant to the Indenture, a holder who elects to convert the 2033 Senior Notes will receive 141.4827 shares of our Common Stock plus such number of additional shares as is applicable on the conversion date per $1,000 principal amount of 2033 Senior Notes based on the early conversion provisions in the Indenture.
We have reviewed all subsequent events and transactions that occurred after the date of our December 31, 2015 Consolidated Balance Sheet date, through the time of filing this Annual Report on Form 10-K.
122
ITEM 9. CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE
None.
ITEM 9A. CONTROLS AND PROCEDURES
Disclosure Controls and Procedures
Our management, with the participation of our Chief Executive Officer and Chief Financial Officer, have evaluated the effectiveness of the Company’s disclosure controls and procedures (as defined in Rules 13a-15(e) and 15d-15(e) under the Securities Exchange Act of 1934, as amended (the “Exchange Act”)) as of December 31, 2015. Our disclosure controls and procedures are designed to provide reasonable assurance that information required to be disclosed by us in the reports that we file or submit under the Exchange Act is recorded, processed, summarized and reported, within the time periods specified in the rules and forms of the Securities and Exchange Commission. Disclosure controls and procedures include, without limitation, controls and procedures designed to ensure that information required to be disclosed by a company in the reports that it files or submits under the Exchange Act is accumulated and communicated to the company’s management, including its principal executive and principal financial officers, as appropriate to allow timely decisions regarding required disclosure. Based on this evaluation, management concluded that our disclosure controls and procedures were effective as of December 31, 2015.
Management’s Annual Report on Internal Control Over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over financial reporting, as such term is defined in Rules 13a-15(e) and 15d-15(e) under the Securities Exchange Act of 1934, as amended. Our internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. All internal control systems, no matter how well designed, have inherent limitations. Therefore, even those systems determined effective could provide only reasonable assurance with respect to financial statement preparation and presentation.
Our management conducted an evaluation of the effectiveness of our internal control over financial reporting as of December 31, 2015, based on the framework in the Internal Control - Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission (the “2013 Internal Control-Integrated Framework”). Based on our evaluation under the framework in 2013 Internal Control-Integrated Framework, our management concluded that our internal control over financial reporting was effective as of December 31, 2015. As permitted, our management’s assessment of and conclusion on the effectiveness of our internal control over financial reporting did not include the internal controls of EirGen Pharma Limited (“EirGen”) or Bio-Reference Laboratories, Inc. (“Bio-Reference”), because they were acquired by us in business combinations in May 2015 and August 2015, respectively. EirGen and Bio-Reference’s assets excluded from the annual assessment process were 15% of consolidated total assets as of December 31, 2015 and 68% of consolidated revenues for the year then ended as a result of the closing of the acquisitions in May 2015 and August 2015.
The effectiveness of the Company’s internal control over financial reporting as of December 31, 2015 has been audited by Ernst & Young LLP, our independent registered public accounting firm, who also audited our Consolidated Financial Statements included in this Annual Report on Form 10-K, as stated in their report which appears with our accompanying Consolidated Financial Statements.
Changes to the Company’s Internal Control Over Financial Reporting
In connection with the acquisitions of EirGen in May 2015 and Bio-Reference in August 2015, we began implementing standards and procedures at EirGen and Bio-Reference, including establishing controls over accounting systems and establishing controls over the preparation of financial statements in accordance with generally accepted accounting principles to ensure that we have in place appropriate internal control over financial reporting at EirGen and Bio-Reference. We are continuing to integrate the acquired operations of EirGen and Bio-Reference into our overall internal control over financial reporting process.
These changes to the Company’s internal control over financial reporting that occurred during the most recent quarter ended December 31, 2015 have materially affected, or are reasonably likely to materially affect, the Company’s internal control over financial reporting.
123
ITEM 9B. OTHER INFORMATION
None.
124
PART III
The information required in Items 10 (Directors, Executive Officers and Corporate Governance), Item 11 (Executive Compensation), Item 12 (Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters), Item 13 (Certain Relationships and Related Transactions, and Director Independence), and Item 14 (Principal Accounting Fees and Services) is incorporated by reference to the Company’s definitive proxy statement for the 2016 Annual Meeting of Stockholders to be filed with the Securities and Exchange Commission within 120 days of December 31, 2015.
125
PART IV.
Item 15. EXHIBITS, FINANCIAL STATEMENT SCHEDULES.
(a) |
(1) |
Financial Statements: See Part II, Item 8 of this report. |
We will file the financial statement schedule entitled "Schedule I - Condensed Financial Information of Registrant" by amendment to this Part IV, Item 15 of this Form 10-K within 30 days. Additionally, the financial statement schedule entitled “Schedule II – Valuation and Qualifying Accounts” has been omitted since the information required is included in the consolidated financial statements and notes thereto. |
||
(2) |
Exhibits: See below. |
|
|
Exhibit
Number
|
Description |
1.1(12)
|
Underwriting Agreement, dated March 9, 2011, by and among OPKO Health, Inc., Jefferies & Company, Inc. and J.P. Morgan Securities LLC, as representatives for the underwriters named therein. |
2.1(1)
|
Merger Agreement and Plan of Reorganization, dated as of March 27, 2007, by and among Acuity Pharmaceuticals, Inc., Froptix Corporation, eXegenics, Inc., e-Acquisition Company I-A, LLC, and e-Acquisition Company II-B, LLC. |
2.2(3)+
|
Securities Purchase Agreement, dated May 2, 2008, by and among Vidus Ocular, Inc., OPKO Instrumentation, LLC, OPKO Health, Inc., and the individual sellers and noteholders named therein. |
2.3(9)
|
Purchase Agreement, dated February 17, 2010, by and among Ignacio Levy García and José de Jesús Levy García, Inmobiliaria Chapalita, S.A. de C.V., Pharmacos Exakta, S.A. de C.V., OPKO Health, Inc., OPKO Health Mexicana S. de R.L. de C.V., and OPKO Manufacturing Facilities S. de R.L. de C.V. |
2.4(14)+
|
Agreement and Plan of Merger, dated January 28, 2011, by and among CURNA Inc., KUR, LLC, OPKO Pharmaceuticals, LLC, OPKO CURNA, LLC, and certain individuals named therein. |
2.5(15)
|
Agreement and Plan of Merger, dated October 13, 2011, by and among OPKO Health, Inc., Claros Merger Subsidiary, LLC, Claros Diagnostics, Inc., and Ellen Baron, Marc Goldberg and Michael Magliochetti on behalf of the Shareholder Representative Committee. |
2.6(17)+
|
Stock Purchase Agreement, dated December 20, 2011, by and among FineTech Pharmaceutical Ltd., Arie Gutman, OPKO Holdings Israel Ltd., and OPKO Health, Inc. |
2.7(18)
|
Purchase Agreement, dated January 20, 2012, by and among OPKO Health, Inc., OPKO Chile S.A., Samuel Alexandre Arama, Inversiones SVJV Limitada, Bruno Sergiani, Inversiones BS Limitada, Pierre-Yves LeGoff, and Inversiones PYTT Limitada. |
2.8(19)+
|
Stock Purchase Agreement, dated August 2, 2012, by and among Farmadiet Group Holding, S.L., the Sellers party thereto, OPKO Health, Inc., and Shebeli XXI, S.L.U. |
2.9(21)+
|
Agreement and Plan of Merger, dated October 18, 2012, by and among Prost-Data, Inc. d/b/a OurLab, Our Labs, Endo Labs and Gold Lab, Jonathan Oppenheimer, M.D., OPKO Health, Inc., OPKO Laboratories Inc., and OPKO Labs, LLC. |
2.10(22)+
|
Share Purchase Agreement, dated January 8, 2013, by among Cytochroma Inc., Cytochroma Holdings ULC, Cytochroma Canada Inc., Cytochroma Development Inc., Proventiv Therapeutics, LLC, Cytochroma Cayman Islands, Ltd., OPKO Health, Inc., and OPKO IP Holdings, Inc. |
2.11(23)
|
Asset Purchase Agreement, dated March 1, 2013, by and between RXi Pharmaceuticals Corporation and OPKO Health, Inc. |
126
2.12(24)
|
Agreement and Plan of Merger, dated April 23, 2013, by and among OPKO Health, Inc., POM Acquisition Inc., and PROLOR Biotech, Inc. |
2.13(28)+
|
Agreement for the Sale and Purchase of Shares in EirGen Pharma Limited, dated May 5, 2015 by and among OPKO Ireland Limited, OPKO Health, Inc. and the Sellers named therein. |
2.14(28)+
|
Form of Additional Agreement for the Sale and Purchase of Shares in EirGen Pharma Limited, dated May 5, 2015 by and among OPKO Ireland Limited and the Sellers named therein. |
2.15(29)+
|
Agreement and Plan of Merger by and among the Company, Bamboo Acquisition, Inc. and Bio-Reference Laboratories, Inc. dated as of June 3, 2015. |
3.1(27)
|
Amended and Restated Certificate of Incorporation, as amended. |
3.2(2)
|
Amended and Restated Bylaws. |
3.3(7)
|
Certificate of Designation of Series D Preferred Stock. |
4.1(1)
|
Form of Common Stock Warrant. |
4.2(7)
|
Form of Common Stock Warrant. |
4.3(25)
|
Indenture, dated January 30, 2013, between OPKO Health, Inc. and Wells Fargo Bank, National Association. |
10.1(1)
|
Form of Lockup Agreement. |
10.2(2)
|
Stock Purchase Agreement, dated December 4, 2007, by and between OPKO Health, Inc. and the members of The Frost Group, LLC. |
10.3(2)*
|
OPKO Health, Inc. 2007 Equity Incentive Plan. |
10.4(26)*
|
Amendment to OPKO Health, Inc. 2007 Equity Incentive Plan. |
10.5(3)
|
Form of Director Indemnification Agreement. |
10.6(3)
|
Form of Officer Indemnification Agreement. |
10.7(4)
|
Stock Purchase Agreement, dated August 8, 2008 by and between OPKO Health, Inc. and the Purchasers named therein. |
10.8(5)
|
Stock Purchase Agreement, dated February 23, 2009 by and between OPKO Health, Inc. and Frost Gamma Investments Trust. |
10.9(6)
|
Form of Stock Purchase Agreement for transactions between OPKO Health, Inc. and Nora Real Estate SA., Vector Group Ltd., Oracle Partners LP, Oracle Institutional Partners, LP., Chung Chia Company Limited, Gold Sino Assets Limited, and Grandtime Associates Limited. |
10.10(6)
|
Stock Purchase Agreement, dated June 10, 2009, by and among OPKO Health, Inc. and Sorrento Therapeutics, Inc. |
10.11(7)
|
Form of Securities Purchase Agreement for Series D Preferred Stock. |
10.12(8)*
|
Form of Restricted Share Award Agreement for Directors. |
127
10.13(8)
|
Cocrystal Discovery, Inc. Agreements. |
10.14(11)
|
Stock Purchase Agreement, dated October 1, 2009, by and among the Laboratoria Volta S.A., Farmacias Ahumada S.A., FASA Chile S.A., OPKO Chile Limitada and Inversones OPKO Limitada, subsidiaries of OPKO Health, Inc. |
10.15(10)+
|
Asset Purchase Agreement, dated October 12, 2009, by and between OPKO Health, Inc. and Schering Corporation. |
10.16(10)
|
Letter Agreement, dated June 29, 2010, by and between OPKO Health, Inc. and Schering Corporation. |
10.17(16)+
|
Exclusive License Agreement by and between TESARO, Inc. and OPKO Health, Inc. dated December 10, 2010. |
10.18(13)
|
Third Amended and Restated Subordinated Note and Security Agreement, dated February 22, 2011, between OPKO Health, Inc. and The Frost Group, LLC. |
10.19(15)+
|
Asset Purchase Agreement dated September 21, 2011, by and among Optos plc, Optos Inc., OPKO Health, Inc., OPKO Instrumentation, LLC, Ophthalmic Technologies, Inc., and OTI (UK) Limited. |
10.20(20)
|
Form of Note Purchase Agreement, dated as of January 25, 2013, by and among OPKO Health, Inc. and each purchaser a party thereto. |
10.21(30)+
|
Development and Commercialization License Agreement by and between OPKO Ireland, Ltd., a subsidiary of OPKO Health, Inc., and Pfizer, Inc. dated December 13, 2014. |
10.22 |
Credit Agreement by and between Bio-Reference Laboratories, Inc. and certain of its subsidiaries and JPMorgan Chase Bank, N.A. dated November 5, 2015. |
21 |
Subsidiaries of the Company. |
23.1 |
Consent of Ernst & Young LLP. |
23.2 |
Consent of MSPC Certified Public Accountants and Advisors, P.C. relating to Bio-Reference Laboratories, Inc.’s financial statements. |
31.1 |
Certification by Phillip Frost, Chief Executive Officer, pursuant to Rule 13a-14(a) and 15d-14(a) of the Securities and Exchange Act of 1934 as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 for the quarterly period ended December 31, 2015. |
31.2 |
Certification by Adam Logal, Chief Financial Officer, pursuant to Rule 13a-14(a) and 15d-14(a) of the Securities and Exchange Act of 1934 as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 for the quarterly period ended December 31, 2015. |
32.1 |
Certification by Phillip Frost, Chief Executive Officer pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 for the quarterly period ended December 31, 2015. |
32.2 |
Certification by Adam Logal, Chief Financial Officer, pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 for the quarterly period ended December 31, 2015. |
99.1(31)
|
The audited consolidated balance sheets of Bio-Reference Laboratories, Inc. and its subsidiaries as of October 31, 2014 and 2013, and the related consolidated statements of operations, shareholders’ equity, and cash flows for each of the years in the three-year period ended October 31, 2014, and the notes and the independent auditor’s reports thereto. |
128
99.2(32)
|
The unaudited consolidated balance sheet of Bio-Reference Laboratories, Inc. and its subsidiaries as of April 30, 2015, the related unaudited consolidated statements of operations, and statements of cash flows for the three and six months ended April 30, 2015, and the notes thereto. |
99.3(33)
|
The unaudited pro forma condensed combined financial statements of the Company and Bio-Reference Laboratories, Inc. |
101.INS |
XBRL Instance Document |
101.SCH |
XBRL Taxonomy Extension Schema Document |
101.CAL |
XBRL Taxonomy Extension Calculation Linkbase Document |
101.DEF |
XBRL Taxonomy Extension Definition Linkbase Document |
101.LAB |
XBRL Taxonomy Extension Label Linkbase Document |
101.PRE |
XBRL Taxonomy Extension Presentation Linkbase Document |
* |
Denotes management contract or compensatory plan or arrangement. |
+ |
Certain confidential material contained in the document has been omitted and filed separately with the Securities and Exchange Commission. |
(1) |
Filed with the Company’s Current Report on Form 8-K filed with the Securities and Exchange Commission on April 2, 2007, and incorporated herein by reference. |
(2) |
Filed with the Company’s Annual Report on Form 10-K filed with the Securities and Exchange Commission on March 31, 2008 and incorporated herein by reference. |
(3) |
Filed with the Company’s Quarterly Report on Form 10-Q filed with the Securities and Exchange Commission on August 8, 2008 for the Company’s three-month period ended June 30, 2008, and incorporated herein by reference. |
(4) |
Filed with the Company’s Quarterly Report on Form 10-Q filed with the Securities and Exchange Commission on November 12, 2008 for the Company’s three-month period ended September 30, 2008, and incorporated herein by reference. |
(5) |
Filed with the Company’s Quarterly Report on Form 10-Q filed with the Securities and Exchange Commission on May 8, 2009 for the Company’s three-month period ended March 31, 2009, and incorporated herein by reference. |
(6) |
Filed with the Company’s Quarterly Report on Form 10-Q filed with the Securities and Exchange Commission on August 7, 2009 for the Company’s three-month period ended June 30, 2009, and incorporated herein by reference. |
(7) |
Filed with the Company’s Current Report on Form 8-K filed with the Securities and Exchange Commission on September 24, 2009, and incorporated herein by reference. |
(8) |
Filed with the Company’s Quarterly Report on Form 10-Q filed with the Securities and Exchange Commission on November 9, 2009 for the Company’s three-month period ended September 30, 2009, and incorporated herein by reference. |
(9) |
Filed with the Company’s Quarterly Report on Form 10-Q filed with the Securities and Exchange Commission on May 10, 2010 for the Company’s three-month period ended March 31, 2010, and incorporated herein by reference. |
(10) |
Filed with the Company’s Amendment to Annual Report on Form 10-K filed with the Securities and Exchange Commission on February 3, 2011. |
(11) |
Filed with the Company’s Annual Report on Form 10-K filed with the Securities and Exchange Commission on March 17, 2010. |
(12) |
Filed with the Company’s Current Report on Form 8-K filed with the Securities and Exchange Commission on March 10, 2011, and incorporated herein by reference. |
(13) |
Filed with the Company’s Quarterly Report on Form 10-Q filed with the Securities and Exchange Commission on May 10, 2011 for the Company’s three-month period ended March 31, 2011, and incorporated herein by reference. |
(14) |
Filed with the Company’s Quarterly Report on Form 10-Q/A filed with the Securities and Exchange Commission on July 5, 2011, and incorporated herein by reference. |
(15) |
Filed with the Company’s Quarterly Report on Form 10-Q filed with the Securities and Exchange Commission on November 9, 2011 for the Company’s three-month period ended September 30, 2011, and incorporated herein by reference. |
(16) |
Filed with the Company’s Annual Report on Form 10-K/A filed with the Securities and Exchange Commission on July 28, 2011. |
129
(17) |
Filed with the Company’s Annual Report on Form 10-K filed with the Securities and Exchange Commission on March 15, 2012. |
(18) |
Filed with the Company’s Quarterly Report on Form 10-Q filed with the Securities and Exchange Commission on May 10, 2012 for the Company’s three-month period ended March 31, 2012, and incorporated herein by reference. |
(19) |
Filed with the Company’s Quarterly Report on Form 10-Q filed with the Securities and Exchange Commission on November 9, 2012 for the Company’s three-month period ended September 30, 2012, and incorporated herein by reference. |
(20) |
Filed with the Company’s Current Report on Form 8-K filed with the Securities and Exchange Commission on January 29, 2013, and incorporated herein by reference. |
(21) |
Filed with the Company’s Annual Report on Form 10-K filed with the Securities and Exchange Commission on March 18, 2013. |
(22) |
Filed with the Company’s Quarterly Report on Form 10-Q filed with the Securities and Exchange Commission on May 10, 2013 for the Company’s three-month period ended March 31, 2013, and incorporated herein by reference. |
(23) |
Filed with the Company’s Schedule 13D filed with the Securities and Exchange Commission on March 22, 2013, and incorporated herein by reference. |
(24) |
Filed as Annex A to the Company’s Preliminary Joint Proxy Statement/Prospectus, Form S-4, with the Securities Exchange Commission on June 27, 2013, as amended, and incorporated herein by reference. |
(25) |
Filed with the Company’s Current Report on Form 8-K filed with the Securities and Exchange Commission on February 5, 2013, and incorporated herein by reference. |
(26) |
Filed with the Company’s Current Report on Form 8-K filed with the Securities Exchange Commission on August 30, 2013, and incorporated herein by reference. |
(27) |
Filed with the Company’s Quarterly Report on Form 10-Q filed with the Securities and Exchange Commission on November 12, 2013 for the Company’s three month period ended September 30, 2013, and incorporated herein by reference. |
(28) |
Filed with the Company’s Quarterly Report on Form 10-Q filed with the Securities and Exchange Commission on August 5, 2015 for the Company’s three month period ended June 30, 2015, and incorporated herein by reference. |
(29) |
Filed with the Company’s Current Report on Form 8-K filed with the Securities and Exchange Commission on June 4, 2015, and incorporated herein by reference. |
(30) |
Filed with the Company’s Annual Report on Form 10-K filed with the Securities and Exchange Commission on February 27, 2015, and incorporated herein by reference. |
(31) |
Filed under Part II, Item 8, of the Bio-Reference Laboratories, Inc. Form 10-K filed with the Securities and Exchange Commission on January 13, 2015 (File No. 0-15266), and incorporated herein by reference. |
(32) |
Filed under Part I, Item 1, of the Bio-Reference Laboratories, Inc. Form 10-Q filed with the Securities and Exchange Commission on June 9, 2015 (File No. 0-15266), and incorporated herein by reference. |
(33) |
Filed under the heading “Unaudited Pro Forma Condensed Combined Financial Statements” beginning on page 27 of the Company’s Registration Statement on Form S-4/A filed with the Securities and Exchange Commission on July 15, 2015 (File No. 333-205480), and incorporated herein by reference. |
130
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
Date: February 29, 2016 |
OPKO HEALTH, INC. |
|
By: |
/s/ Phillip Frost, M.D. |
|
Phillip Frost, M.D. |
||
Chairman of the Board and |
||
Chief Executive Officer |
||
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
Signature |
Title |
Date |
||
/s/ Phillip Frost, M.D. |
Chairman of the Board and Chief Executive |
February 29, 2016 |
||
Phillip Frost, M.D. |
Officer (Principal Executive Officer) |
|||
/s/ Jane H. Hsiao, Ph.D., MBA |
Vice Chairman and Chief Technical Officer |
February 29, 2016 |
||
Jane H. Hsiao, Ph.D., MBA |
||||
/s/ Steven D. Rubin |
Director and Executive Vice President – |
February 29, 2016 |
||
Steven D. Rubin |
Administration |
|||
/s/ Adam Logal |
Senior Vice President, Chief Financial Officer, |
February 29, 2016 |
||
Adam Logal |
Chief Accounting Officer and Treasurer
(Principal Financial Officer)
|
|||
/s/ Robert Baron |
Director |
February 29, 2016 |
||
Robert Baron |
||||
/s/ Thomas E. Beier |
Director |
February 29, 2016 |
||
Thomas E. Beier |
||||
/s/ Dmitry Kolosov |
Director |
February 29, 2016 |
||
Dmitry Kolosov |
||||
/s/ Richard A. Lerner, M.D. |
Director |
February 29, 2016 |
||
Richard A. Lerner, M.D. |
||||
/s/ John A. Paganelli |
Director |
February 29, 2016 |
||
John A. Paganelli |
||||
/s/ Richard C. Pfenniger, Jr. |
Director |
February 29, 2016 |
||
Richard C. Pfenniger, Jr. |
||||
/s/ Alice Lin-Tsing Yu, M.D., Ph.D. |
Director |
February 29, 2016 |
||
Alice Lin-Tsing Yu, M.D., Ph.D. |
||||
131
Exhibit Index
Exhibit Number |
Description |
10.22 |
Credit Agreement by and between Bio-Reference Laboratories, Inc. and certain of its subsidiaries and JPMorgan Chase Bank, N.A. dated November 5, 2015. |
21 |
Subsidiaries of the Company. |
23.1 |
Consent of Ernst & Young LLP. |
23.2 |
Consent of MSPC Certified Public Accountants and Advisors, P.C. relating to Bio-Reference Laboratories, Inc.’s financial statements. |
31.1 |
Certification by Phillip Frost, Chief Executive Officer, pursuant to Rule 13a-14(a) and 15d-14(a) of the Securities and Exchange Act of 1934 as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 for the quarterly period ended December 31, 2015. |
31.2 |
Certification by Adam Logal, Chief Financial Officer, pursuant to Rule 13a-14(a) and 15d-14(a) of the Securities and Exchange Act of 1934 as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 for the quarterly period ended December 31, 2015. |
32.1 |
Certification by Phillip Frost, Chief Executive Officer pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 for the quarterly period ended December 31, 2015. |
32.2 |
Certification by Adam Logal, Chief Financial Officer, pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 for the quarterly period ended December 31, 2015. |
101.INS |
XBRL Instance Document |
101.SCH |
XBRL Taxonomy Extension Schema Document |
101.CAL |
XBRL Taxonomy Extension Calculation Linkbase Document |
101.DEF |
XBRL Taxonomy Extension Definition Linkbase Document |
101.LAB |
XBRL Taxonomy Extension Label Linkbase Document |
101.PRE |
XBRL Taxonomy Extension Presentation Linkbase Document |
132